

What Does Lesion Blood Flow Tell Us About Risk Stratification and Successful Management of Non-variceal UGI Bleeding?
- PMID: 28374310
- PMCID: PMC6018027
- DOI: 10.1007/s11894-017-0556-y
What Does Lesion Blood Flow Tell Us About Risk Stratification and Successful Management of Non-variceal UGI Bleeding?
Abstract
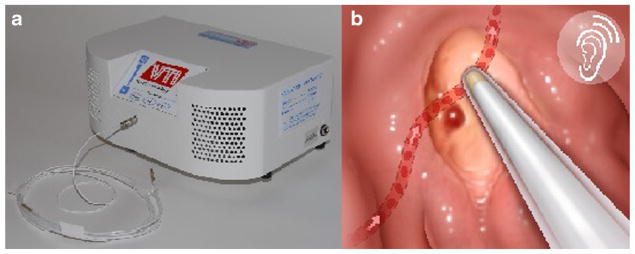
Purpose of review: There has been a decline in mortality associated with upper gastrointestinal (UGI) hemorrhage as the use of urgent endoscopy has increased. This review will examine endoscopic risk stratification of non-variceal UGI bleeding (e.g., ulcers, Dieulafoy lesions, and Mallory-Weiss tears), including the use of the Doppler endoscopic probe (DEP).
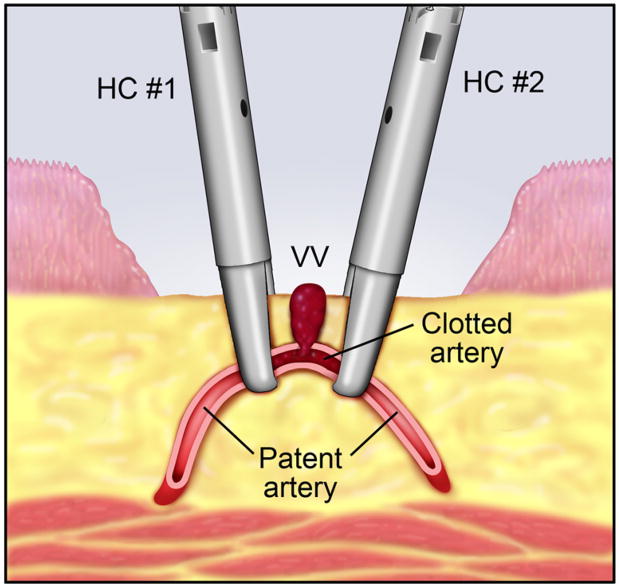
Recent findings: Prospective studies evaluating the use of DEP in non-variceal UGI hemorrhage showed that lesions with high-risk stigmata of recent hemorrhage (SRH) have a higher rate of a positive DEP signal compared to those with intermediate-risk SRH. Additionally, lesions with a persistently positive DEP signal after endoscopic hemostasis were seen with high-risk SRH and had a higher 30-day rebleeding rate. Residual arterial blood flow underneath ulcers is a significant risk factor for rebleeding. However, if more endoscopic treatment is applied, clinical outcomes for patients with severe non-variceal UGI hemorrhage are improved, as documented by a recent CURE Hemostasis randomized controlled trial (RCT).
Keywords: Doppler endoscopic probe; Risk stratification; Upper gastrointestinal bleeding.
Figures
Similar articles
-
The Cutting Edge: Doppler Probe in Guiding Endoscopic Hemostasis.Gastrointest Endosc Clin N Am. 2018 Jul;28(3):321-330. doi: 10.1016/j.giec.2018.02.005. Gastrointest Endosc Clin N Am. 2018. PMID: 29933778 Review.
-
Doppler Endoscopic Probe Monitoring of Blood Flow Improves Risk Stratification and Outcomes of Patients With Severe Nonvariceal Upper Gastrointestinal Hemorrhage.Gastroenterology. 2017 May;152(6):1310-1318.e1. doi: 10.1053/j.gastro.2017.01.042. Epub 2017 Feb 4. Gastroenterology. 2017. PMID: 28167214 Free PMC article. Clinical Trial.
-
The Importance of Arterial Blood Flow Detection for Risk Stratification and Eradication to Achieve Definitive Hemostasis of Severe Non-Variceal UGI Hemorrhage.J Clin Med. 2023 Oct 11;12(20):6473. doi: 10.3390/jcm12206473. J Clin Med. 2023. PMID: 37892610 Free PMC article.
-
Doppler endoscopic probe as a guide to risk stratification and definitive hemostasis of peptic ulcer bleeding.Gastrointest Endosc. 2016 Jan;83(1):129-36. doi: 10.1016/j.gie.2015.07.012. Epub 2015 Aug 28. Gastrointest Endosc. 2016. PMID: 26318834 Free PMC article.
-
Nonvariceal Upper Gastrointestinal Bleeding: Timing of Endoscopy and Ways to Improve Endoscopic Visualization.Gastrointest Endosc Clin N Am. 2015 Jul;25(3):443-8. doi: 10.1016/j.giec.2015.03.002. Gastrointest Endosc Clin N Am. 2015. PMID: 26142030 Review.
Cited by
-
The effect of pantoprazole and somatostatin combined with thrombin in the treatment of non-esophagogastric varicosity upper gastrointestinal bleeding.Am J Transl Res. 2021 May 15;13(5):5484-5490. eCollection 2021. Am J Transl Res. 2021. PMID: 34150147 Free PMC article.
References
-
- Forrest JA, Finlayson ND, Shearman DJ. Endoscopy in gastrointestinal bleeding. Lancet. 1974;2:394–7. - PubMed
-
- Jensen DM, Ohning GV, Kovacs TOG, Ghassemi KA, Jutabha R, Dulai GS, et al. Doppler endoscopic probe as a guide to risk stratification and definitive hemostasis of peptic ulcer bleeding. Gastrointest Endosc. 2016;83:129–36. doi: 10.1016/j.gie.2015.07.012. Shows that DEP can further stratify risk of rebleeding after standard, visually-guided endoscopic hemostasis. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
