

Autoimmune Pancreatitis in Children: Characteristic Features, Diagnosis, and Management
- PMID: 28374818
- PMCID: PMC5908471
- DOI: 10.1038/ajg.2017.85
Autoimmune Pancreatitis in Children: Characteristic Features, Diagnosis, and Management
Abstract
Objectives: Autoimmune pancreatitis (AIP) is an increasingly recognized disease entity, but data in children are limited. AIP presentation and outcome in children might differ from the adult experience. We aim to determine the characteristic features of AIP in children.
Methods: Data about clinical symptoms, imaging, histology, and treatment were collected using two sources: (i) a systematic literature search and (ii) the INSPPIRE database, the largest international multicenter study of pancreatitis in children and the Cliniques Universitaires St-Luc (CUSL) registry.
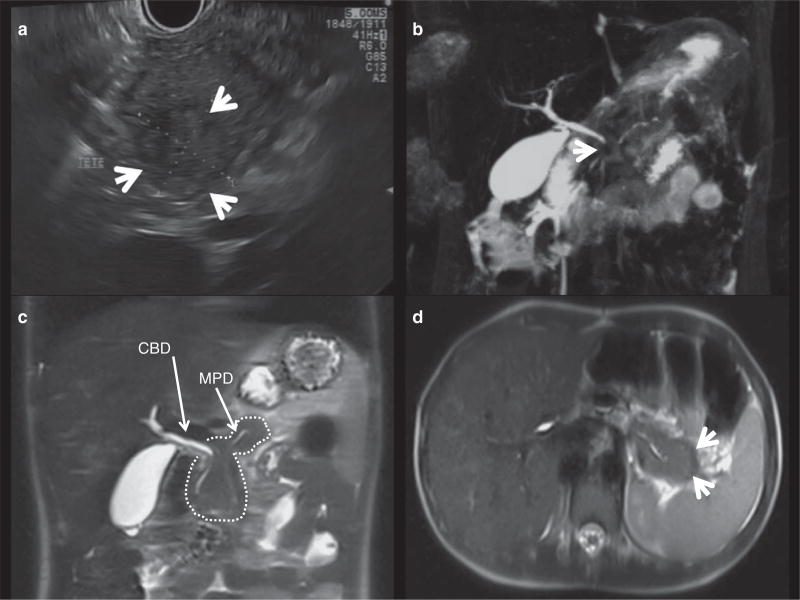
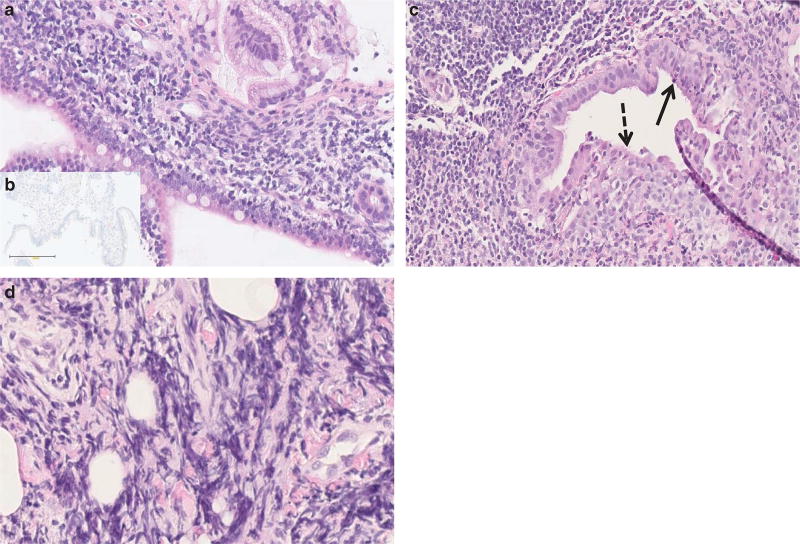
Results: We identified 48 AIP cases: 30 from literature review, 14 from INSPPIRE, and 4 from CUSL. The median age at diagnosis was 13 years (range 2-17 years). Abdominal pain (43/47, 91%) and/or obstructive jaundice (20/47, 42%) were the most common symptoms at diagnosis. Elevated serum IgG4 levels were only observed in 9/40 (22%) children. Cross-sectional imaging studies were abnormal in all children including hypointense global or focal gland enlargement (39/47, 83%), main pancreatic duct irregularity (30/47, 64%), and common bile duct stricture (26/47, 55%). A combination of lymphoplasmacytic inflammation, pancreatic fibrosis, and ductal granulocyte infiltration were the main histological findings (18/25, 72%). Children with AIP had a prompt clinical response to steroids. Complications of AIP included failure of exocrine (4/25, 16%) and endocrine (3/27, 11%) pancreas function.
Conclusions: Pediatric AIP has a distinct presentation with features similar to type 2 AIP in adults. This comprehensive report on the largest group of children with AIP to date is expected to help with the diagnosis and management of this disease and pave the way for future research studies.
Conflict of interest statement
Figures
References
-
- Sarles H, Sarles JC, Muratore R, et al. Chronic inflammatory sclerosis of the pancreas--an autonomous pancreatic disease? Am J Dig Dis. 1961;6:688–98. - PubMed
-
- Yoshida K, Toki F, Takeuchi T, et al. Chronic pancreatitis caused by an auto- immune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci. 1995;40:1561–8. - PubMed
-
- Shimosegawa T, Chari ST, Frulloni L, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas. 2011;40:352–8. - PubMed
-
- Hart PA, Zen Y, Chari ST. Recent advances in autoimmune pancreatitis. Gastroenterology. 2015;149:39–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
