

Cause-specific Mortality in a Population-based Cohort of 9799 Women Treated for Ductal Carcinoma In Situ
- PMID: 28375855
- PMCID: PMC5916471
- DOI: 10.1097/SLA.0000000000002239
Cause-specific Mortality in a Population-based Cohort of 9799 Women Treated for Ductal Carcinoma In Situ
Abstract
Objective: To assess cause-specific mortality in women treated for ductal carcinoma in situ (DCIS).
Background: From screening and treatment perspective, it is relevant to weigh the low breast cancer mortality after DCIS against mortality from other causes and expected mortality in the general population.
Methods: We conducted a population-based cohort study comprising 9799 Dutch women treated for primary DCIS between 1989 and 2004 and estimated standardized mortality ratios (SMRs).
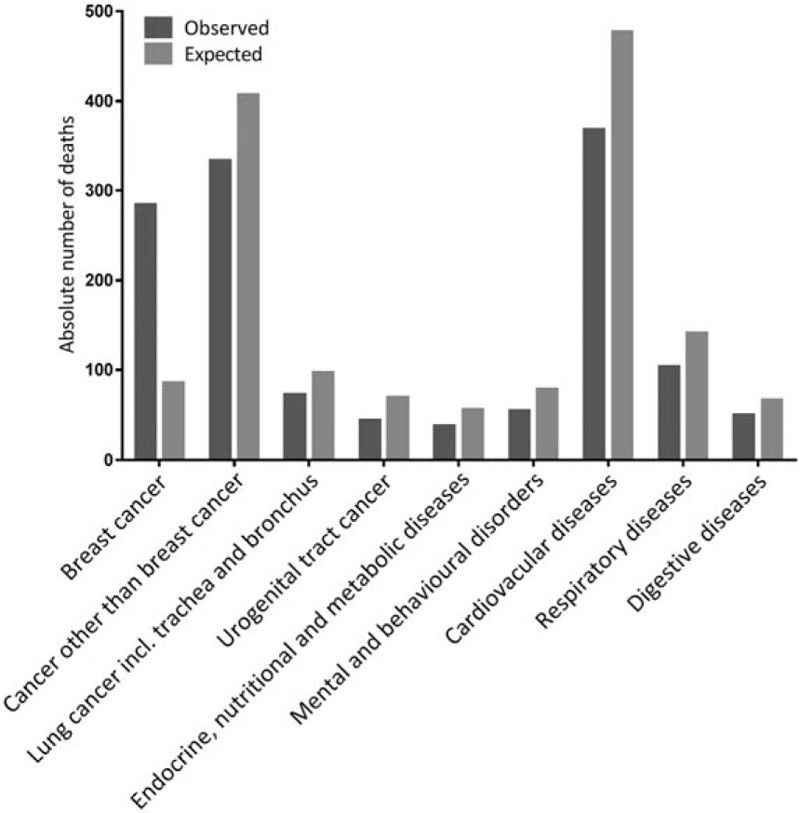
Results: After a median follow up of 9.8 years, 1429 patients had died of whom 284 caused by breast cancer (2.9% of total cohort). DCIS patients <50 years experienced higher mortality compared with women in the general population (SMR 1.7; 95% confidence interval, CI: 1.4-2.0), whereas patients >50 had significantly lower mortality (SMR 0.9; 95% CI: 0.8-0.9). Overall, the risk of dying from general diseases and cancer other than breast cancer was lower than in the general population, whereas breast cancer mortality was increased. The SMR for breast cancer decreased from 7.5 (95% CI: 5.9-9.3) to 2.8 (95% CI: 2.4-3.2) for women aged <50 and >50 years, respectively. The cumulative breast cancer mortality 10 years after DCIS was 2.3% for women <50 years and 1.4% for women >50 years treated for DCIS between 1999 and 2004.
Conclusions: DCIS patients >50 years had lower risk of dying from all causes combined compared with the general female population, which may reflect differences in health behavior. Women with DCIS had higher risk of dying from breast cancer than the general population, but absolute 10-year risks were low.
Conflict of interest statement
BCS indicates breast conserving surgery; CI, confidence interval; DCIS, ductal carcinoma in situ; NA, not applicable; RT, radiotherapy; SHR, subdistribution hazard ratio (with death due to other causes as a competing event).
Model 1: adjusted for age at DCIS diagnosis, period of DCIS diagnosis and DCIS grade.
Model 2: adjusted for age at DCIS diagnosis, period of DCIS diagnosis, DCIS grade and subsequent invasive breast cancer; with subsequent ipsilateral and contralateral invasive breast cancer as time-dependent variables.
Figures

Comment in
-
DCIS and Breast Cancer: Challenging the Paradigm.Ann Surg. 2018 Jul;268(1):e17. doi: 10.1097/SLA.0000000000002417. Ann Surg. 2018. PMID: 28697051 No abstract available.
-
Response to: "DCIS and Breast Cancer: Challenging the Paradigm".Ann Surg. 2018 Jul;268(1):e18. doi: 10.1097/SLA.0000000000002418. Ann Surg. 2018. PMID: 28697052 No abstract available.
References
-
- Lopez-Garcia MA, Geyer FC, Lacroix-Triki M, et al. Breast cancer precursors revisited: molecular features and progression pathways. Histopathology 2010; 57:171–192. - PubMed
-
- Erbas B, Provenzano E, Armes J, et al. The natural history of ductal carcinoma in situ of the breast: a review. Breast Cancer Res Treat 2006; 97:135–144. - PubMed
-
- Ernster VL, Barclay J, Kerlikowske K, et al. Mortality among women with ductal carcinoma in situ of the breast in the population-based surveillance, epidemiology, and end results program. Arch Intern Med 2000; 160:953–958. - PubMed
-
- Narod SA, Iqbal J, Giannakeas V, et al. Breast cancer mortality after a diagnosis of ductal carcinoma in situ. JAMA Oncol 2015; 1:888–896. - PubMed
-
- Bartlett JMS, Nofech-Moses S, Rakovitch E. Ductal carcinoma in situ of the breast: can biomarkers improve current management? Clin Chem 2014; 60:60–67. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
