

Demographic transition and the dynamics of measles in six provinces in China: A modeling study
- PMID: 28376084
- PMCID: PMC5380361
- DOI: 10.1371/journal.pmed.1002255
Demographic transition and the dynamics of measles in six provinces in China: A modeling study
Abstract
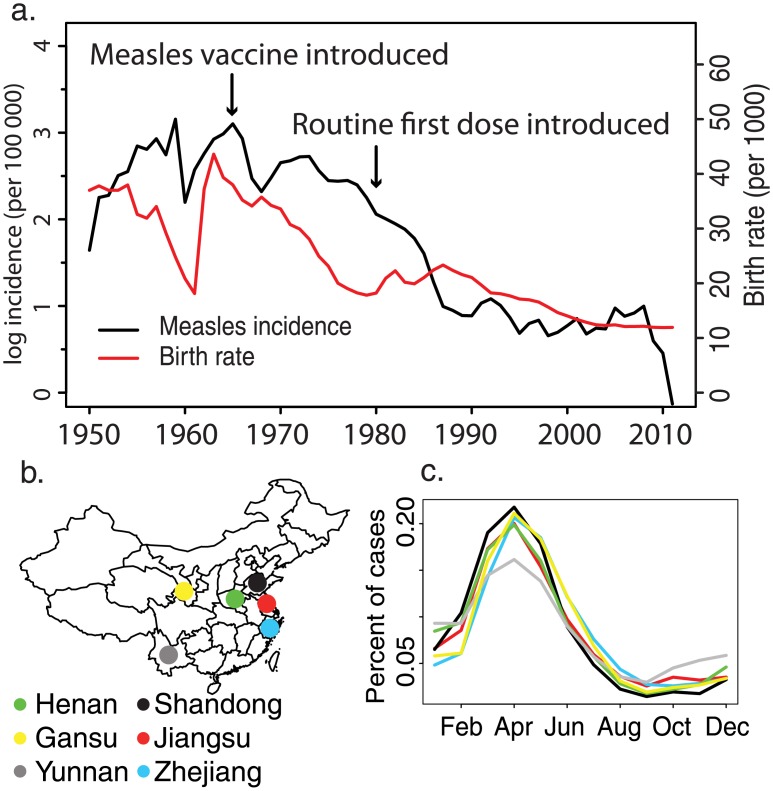
Background: Industrialization and demographic transition generate nonstationary dynamics in human populations that can affect the transmission and persistence of infectious diseases. Decades of increasing vaccination and development have led to dramatic declines in the global burden of measles, but the virus remains persistent in much of the world. Here we show that a combination of demographic transition, as a result of declining birth rates, and reduced measles prevalence, due to improved vaccination, has shifted the age distribution of susceptibility to measles throughout China.
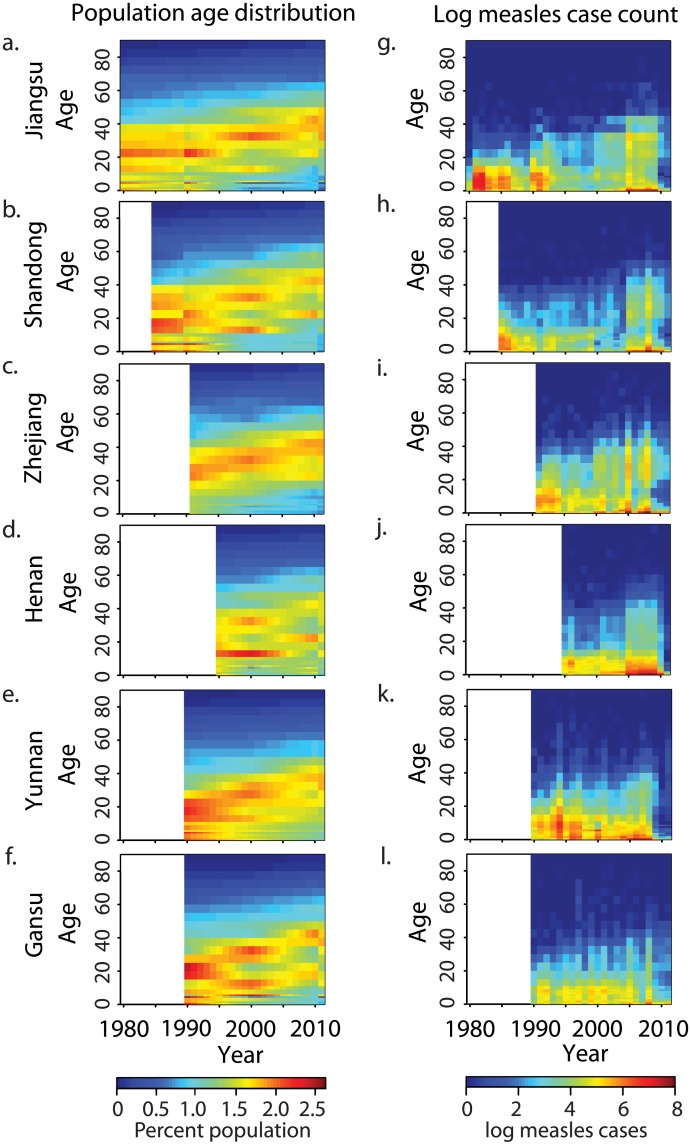
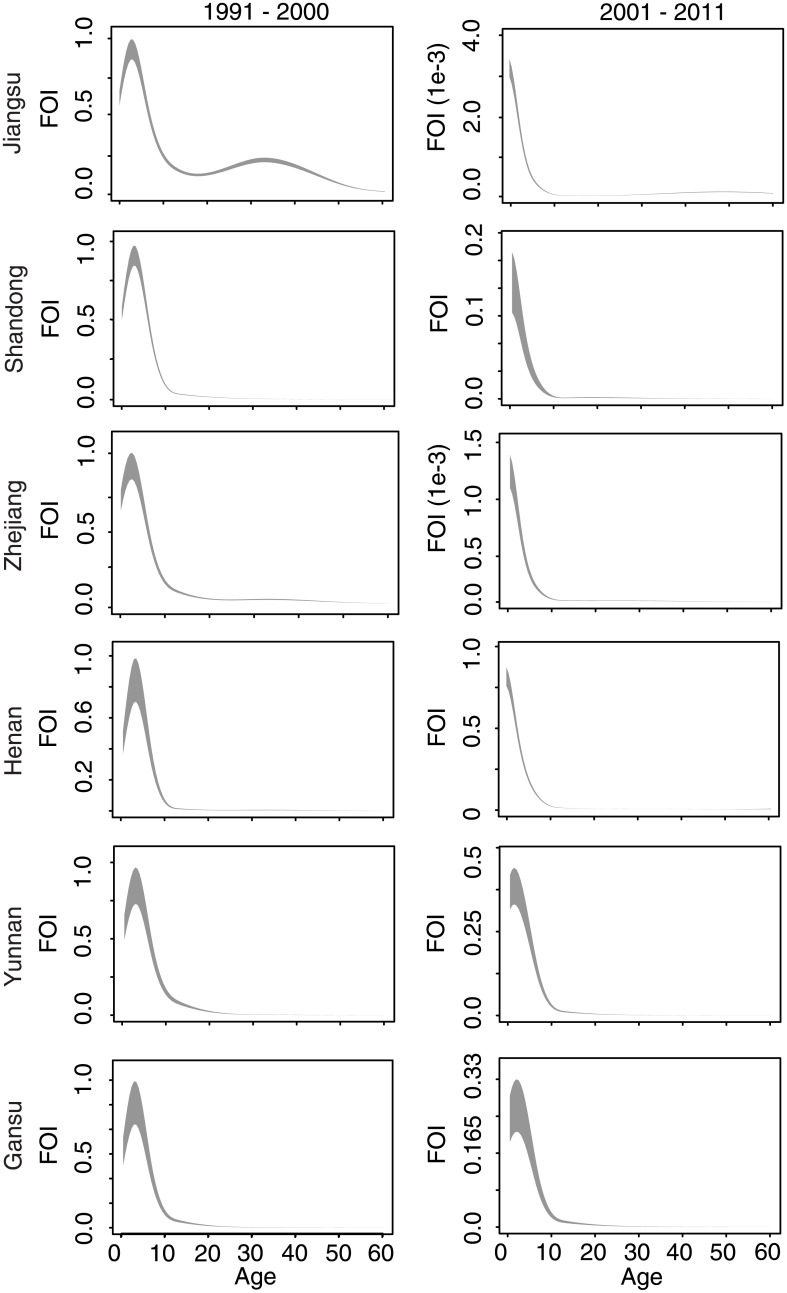
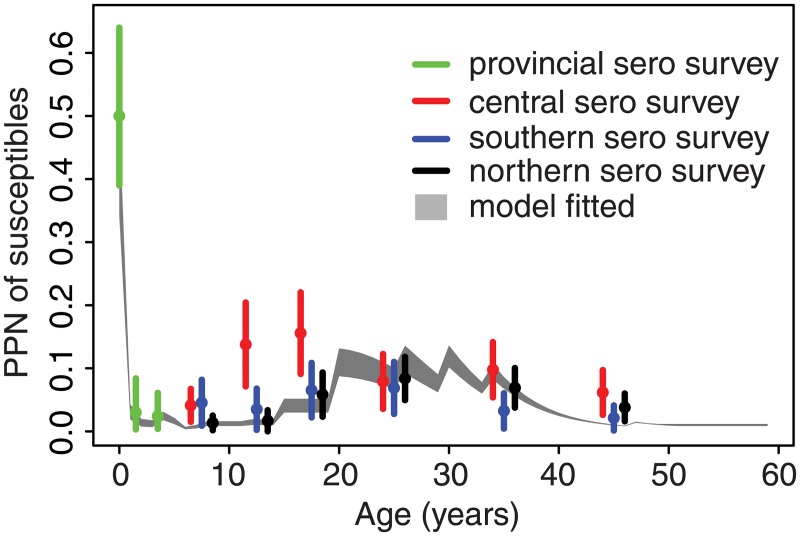
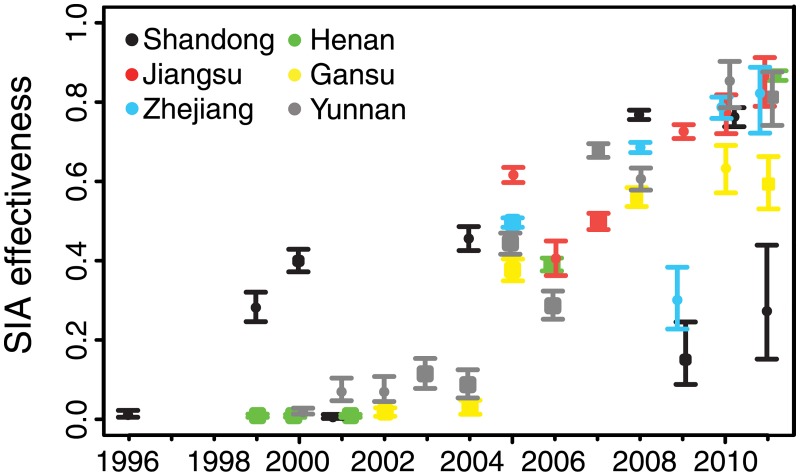
Methods and findings: We fit a novel time-varying catalytic model to three decades of age-specific measles case reporting in six provinces in China to quantify the change in the age-specific force of infection for measles virus over time. We further quantified the impact of supplemental vaccination campaigns on the reduction of susceptible individuals. The force of infection of measles has declined dramatically (90%-97% reduction in transmission rate) in three industrialized eastern provinces during the last decade, driving a concomitant increase in both the relative proportion and absolute number of adult cases, while three central and western provinces exhibited dynamics consistent with endemic persistence (24%-73% reduction in transmission rate). The reduction in susceptible individuals due to supplemental vaccination campaigns is frequently below the nominal campaign coverage, likely because campaigns necessarily vaccinate those who may already be immune. The impact of these campaigns has significantly improved over time: campaigns prior to 2005 were estimated to have achieved less than 50% reductions in the proportion susceptible in the target age classes, but campaigns from 2005 onwards reduced the susceptible proportion by 32%-87%. A limitation of this study is that it relies on case surveillance, and thus inference may be biased by age-specific variation in measles reporting.
Conclusions: The age distribution of measles cases changes in response to both demographic and vaccination processes. Combining both processes in a novel catalytic model, we illustrate that age-specific incidence patterns reveal regional differences in the progress to measles elimination and the impact of vaccination controls in China. The shift in the age distribution of measles susceptibility in response to demographic and vaccination processes emphasizes the importance of progressive control strategies and measures to evaluate program success that anticipate and react to this transition in observed incidence.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Characteristics of measles epidemics in China (1951-2004) and implications for elimination: A case study of three key locations.PLoS Comput Biol. 2019 Feb 4;15(2):e1006806. doi: 10.1371/journal.pcbi.1006806. eCollection 2019 Feb. PLoS Comput Biol. 2019. PMID: 30716080 Free PMC article.
-
Deciphering the relative weights of demographic transition and vaccination in the decrease of measles incidence in Italy.Proc Biol Sci. 2014 Jan 8;281(1777):20132676. doi: 10.1098/rspb.2013.2676. Print 2014 Feb 22. Proc Biol Sci. 2014. PMID: 24403333 Free PMC article.
-
Evaluating vaccination policies to accelerate measles elimination in China: a meta-population modelling study.Int J Epidemiol. 2019 Aug 1;48(4):1240-1251. doi: 10.1093/ije/dyz058. Int J Epidemiol. 2019. PMID: 30977801 Free PMC article.
-
[Vaccination coverage against measles and sero-epidemiology of measles-specific IgG antibodies in German children and adolescents].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013 Sep;56(9):1243-52. doi: 10.1007/s00103-013-1790-6. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013. PMID: 23990086 Review. German.
-
Prospects for the eradication of infectious diseases.Rev Infect Dis. 1984 May-Jun;6(3):405-11. doi: 10.1093/clinids/6.3.405. Rev Infect Dis. 1984. PMID: 6377445 Review.
Cited by
-
Incorporating human dynamic populations in models of infectious disease transmission: a systematic review.BMC Infect Dis. 2022 Nov 18;22(1):862. doi: 10.1186/s12879-022-07842-0. BMC Infect Dis. 2022. PMID: 36401210 Free PMC article.
-
Modeling the impact of changes in day-care contact patterns on the dynamics of varicella transmission in France between 1991 and 2015.PLoS Comput Biol. 2018 Aug 1;14(8):e1006334. doi: 10.1371/journal.pcbi.1006334. eCollection 2018 Aug. PLoS Comput Biol. 2018. PMID: 30067732 Free PMC article.
-
Estimation and prediction for a mechanistic model of measles transmission using particle filtering and maximum likelihood estimation.Stat Med. 2019 Sep 20;38(21):4146-4158. doi: 10.1002/sim.8290. Epub 2019 Jul 9. Stat Med. 2019. PMID: 31290184 Free PMC article.
-
A Serological Survey of Measles and Rubella Antibodies among Different Age Groups in Eastern China.Vaccines (Basel). 2024 Jul 25;12(8):842. doi: 10.3390/vaccines12080842. Vaccines (Basel). 2024. PMID: 39203968 Free PMC article.
-
Comparative study on molecular epidemiology of measles H1 outbreak and sporadic cases in Shandong Province, 2013-2019.BMC Genomics. 2022 Apr 14;23(1):305. doi: 10.1186/s12864-022-08492-x. BMC Genomics. 2022. PMID: 35421927 Free PMC article.
References
-
- Cliff AD, Haggett P, Smallman-Raynor M. Measles: an historical geography of a major human viral disease from global expansion to local retreat, 1840–1990. Oxford: Blackwell; 1993. 462 p.
-
- European Center for Disease Prevention and Control. Annual epidemiological report 2013. Stockholm: European Center for Disease Prevention and Control; 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
