

Can machine-learning improve cardiovascular risk prediction using routine clinical data?
- PMID: 28376093
- PMCID: PMC5380334
- DOI: 10.1371/journal.pone.0174944
Can machine-learning improve cardiovascular risk prediction using routine clinical data?
Abstract
Background: Current approaches to predict cardiovascular risk fail to identify many people who would benefit from preventive treatment, while others receive unnecessary intervention. Machine-learning offers opportunity to improve accuracy by exploiting complex interactions between risk factors. We assessed whether machine-learning can improve cardiovascular risk prediction.
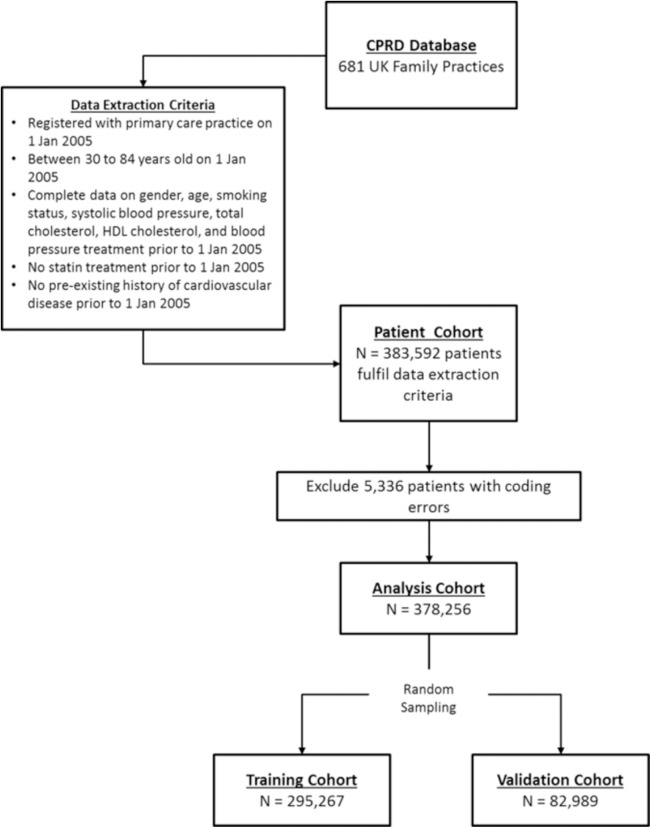
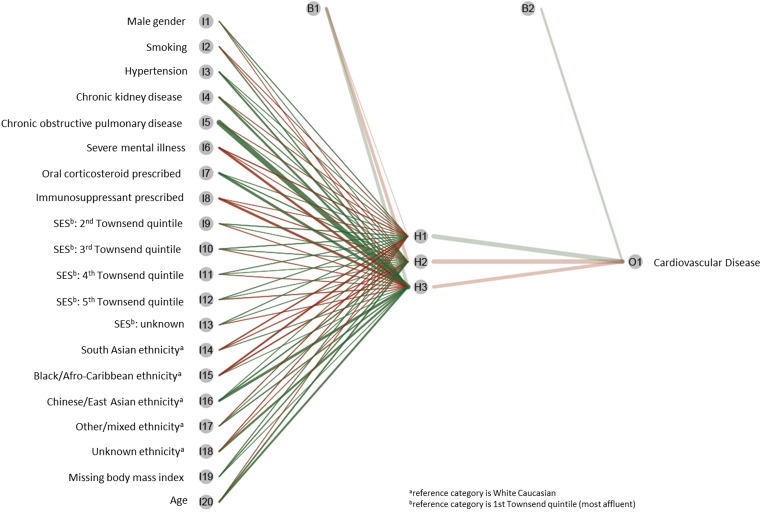
Methods: Prospective cohort study using routine clinical data of 378,256 patients from UK family practices, free from cardiovascular disease at outset. Four machine-learning algorithms (random forest, logistic regression, gradient boosting machines, neural networks) were compared to an established algorithm (American College of Cardiology guidelines) to predict first cardiovascular event over 10-years. Predictive accuracy was assessed by area under the 'receiver operating curve' (AUC); and sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) to predict 7.5% cardiovascular risk (threshold for initiating statins).
Findings: 24,970 incident cardiovascular events (6.6%) occurred. Compared to the established risk prediction algorithm (AUC 0.728, 95% CI 0.723-0.735), machine-learning algorithms improved prediction: random forest +1.7% (AUC 0.745, 95% CI 0.739-0.750), logistic regression +3.2% (AUC 0.760, 95% CI 0.755-0.766), gradient boosting +3.3% (AUC 0.761, 95% CI 0.755-0.766), neural networks +3.6% (AUC 0.764, 95% CI 0.759-0.769). The highest achieving (neural networks) algorithm predicted 4,998/7,404 cases (sensitivity 67.5%, PPV 18.4%) and 53,458/75,585 non-cases (specificity 70.7%, NPV 95.7%), correctly predicting 355 (+7.6%) more patients who developed cardiovascular disease compared to the established algorithm.
Conclusions: Machine-learning significantly improves accuracy of cardiovascular risk prediction, increasing the number of patients identified who could benefit from preventive treatment, while avoiding unnecessary treatment of others.
Conflict of interest statement
Figures
References
-
- World Health Organization. Global Status Report on Noncommunicable Diseases Geneva, Switzerland: World Health Organization, 2014.
-
- Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 135(11): 1–50. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
