

Risk prediction models for selection of lung cancer screening candidates: A retrospective validation study
- PMID: 28376113
- PMCID: PMC5380315
- DOI: 10.1371/journal.pmed.1002277
Risk prediction models for selection of lung cancer screening candidates: A retrospective validation study
Erratum in
-
Correction: Risk prediction models for selection of lung cancer screening candidates: A retrospective validation study.PLoS Med. 2020 Sep 25;17(9):e1003403. doi: 10.1371/journal.pmed.1003403. eCollection 2020 Sep. PLoS Med. 2020. PMID: 32976487 Free PMC article.
Abstract
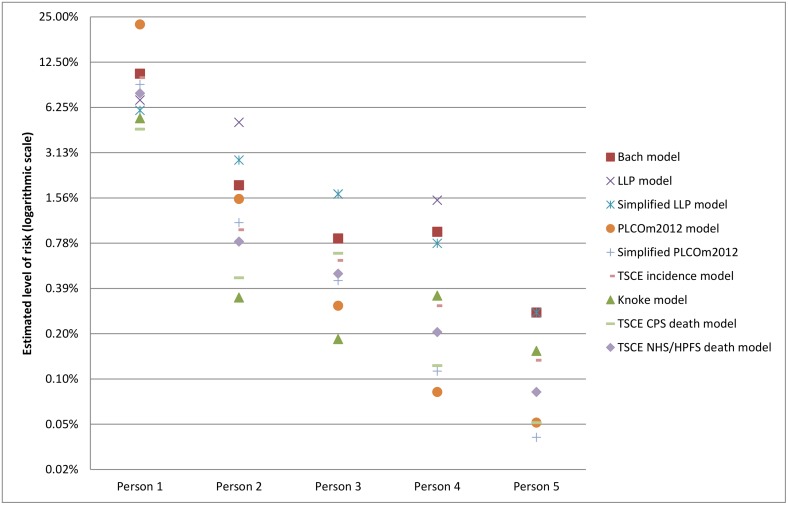
Background: Selection of candidates for lung cancer screening based on individual risk has been proposed as an alternative to criteria based on age and cumulative smoking exposure (pack-years). Nine previously established risk models were assessed for their ability to identify those most likely to develop or die from lung cancer. All models considered age and various aspects of smoking exposure (smoking status, smoking duration, cigarettes per day, pack-years smoked, time since smoking cessation) as risk predictors. In addition, some models considered factors such as gender, race, ethnicity, education, body mass index, chronic obstructive pulmonary disease, emphysema, personal history of cancer, personal history of pneumonia, and family history of lung cancer.
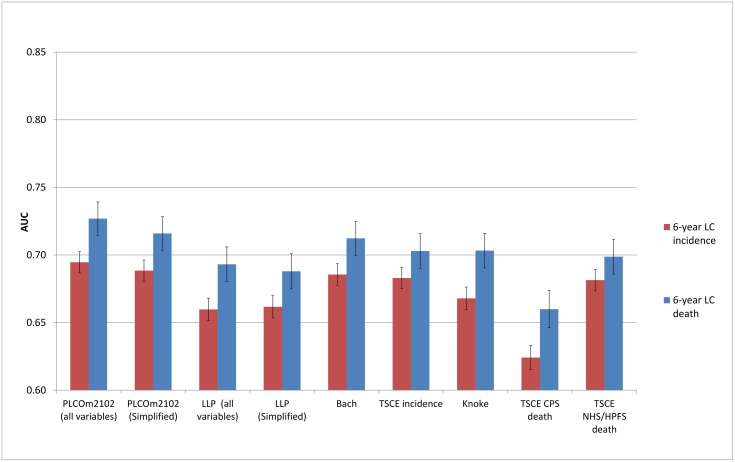
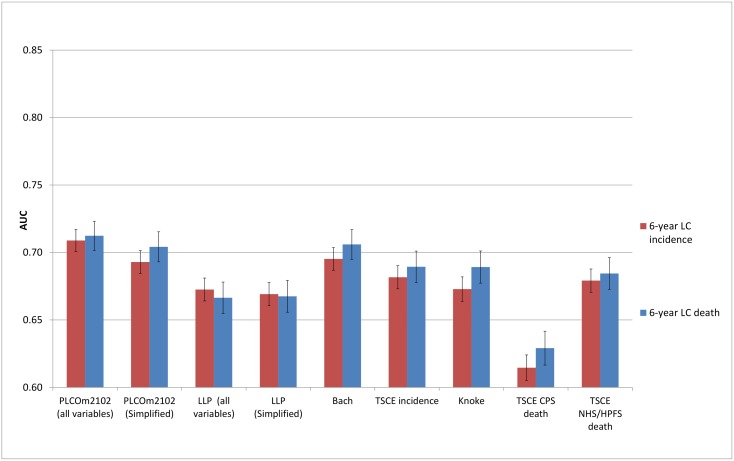
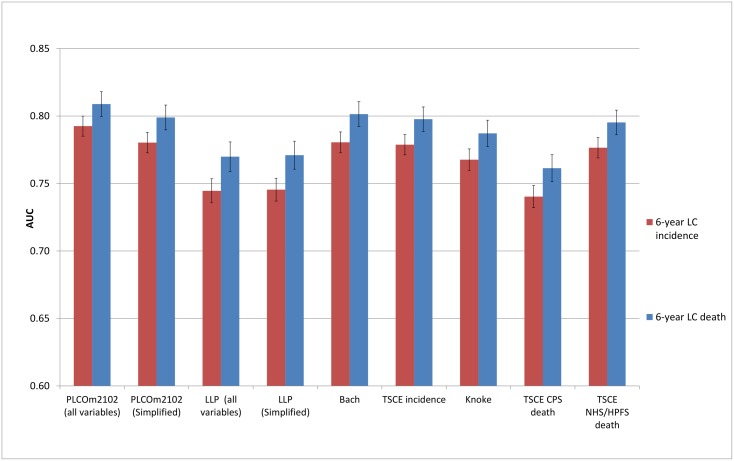
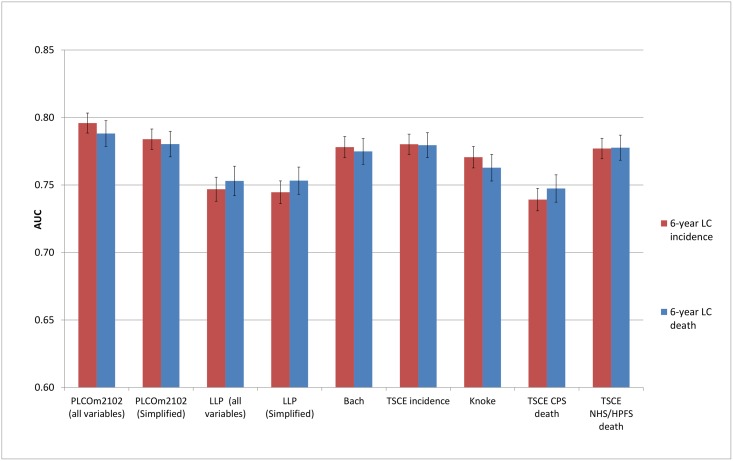
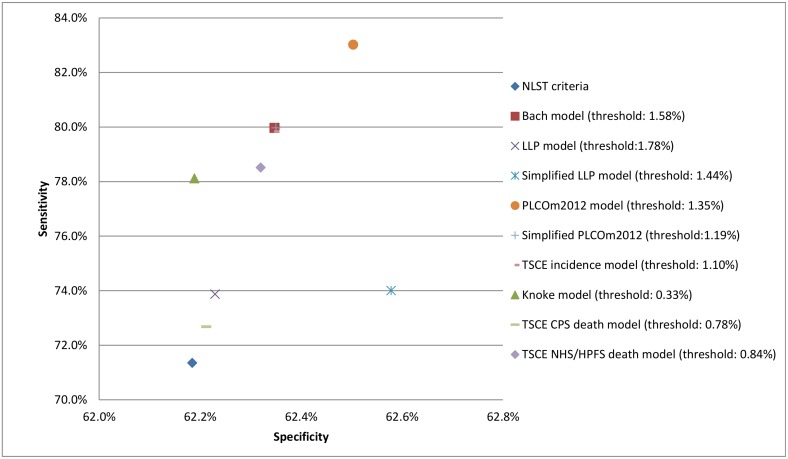
Methods and findings: Retrospective analyses were performed on 53,452 National Lung Screening Trial (NLST) participants (1,925 lung cancer cases and 884 lung cancer deaths) and 80,672 Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial (PLCO) ever-smoking participants (1,463 lung cancer cases and 915 lung cancer deaths). Six-year lung cancer incidence and mortality risk predictions were assessed for (1) calibration (graphically) by comparing the agreement between the predicted and the observed risks, (2) discrimination (area under the receiver operating characteristic curve [AUC]) between individuals with and without lung cancer (death), and (3) clinical usefulness (net benefit in decision curve analysis) by identifying risk thresholds at which applying risk-based eligibility would improve lung cancer screening efficacy. To further assess performance, risk model sensitivities and specificities in the PLCO were compared to those based on the NLST eligibility criteria. Calibration was satisfactory, but discrimination ranged widely (AUCs from 0.61 to 0.81). The models outperformed the NLST eligibility criteria over a substantial range of risk thresholds in decision curve analysis, with a higher sensitivity for all models and a slightly higher specificity for some models. The PLCOm2012, Bach, and Two-Stage Clonal Expansion incidence models had the best overall performance, with AUCs >0.68 in the NLST and >0.77 in the PLCO. These three models had the highest sensitivity and specificity for predicting 6-y lung cancer incidence in the PLCO chest radiography arm, with sensitivities >79.8% and specificities >62.3%. In contrast, the NLST eligibility criteria yielded a sensitivity of 71.4% and a specificity of 62.2%. Limitations of this study include the lack of identification of optimal risk thresholds, as this requires additional information on the long-term benefits (e.g., life-years gained and mortality reduction) and harms (e.g., overdiagnosis) of risk-based screening strategies using these models. In addition, information on some predictor variables included in the risk prediction models was not available.
Conclusions: Selection of individuals for lung cancer screening using individual risk is superior to selection criteria based on age and pack-years alone. The benefits, harms, and feasibility of implementing lung cancer screening policies based on risk prediction models should be assessed and compared with those of current recommendations.
Conflict of interest statement
HJdK and KtH are members of the Cancer Intervention and Surveillance Modeling Network (CISNET) Lung working group (grant 1U01CA199284-01 from NIH). HJdK is the principal investigator of the Dutch-Belgian Lung Cancer Screening Trial (Nederlands-Leuvens Longkanker Screenings onderzoek; the NELSON trial). KtH is a researcher affiliated with the NELSON trial. HJdK and KtH received a grant from the University of Zurich to assess the cost-effectiveness of computed tomographic lung cancer screening in Switzerland. HJdK took part in a 1-day advisory meeting on biomarkers organized by M.D. Anderson/Health Sciences during the 16th World Conference on Lung Cancer. HJdK and KtH were involved in a Health Technology Assessment study for CT Lung Cancer Screening in Canada (dr. Paszat, Cancer Care Ontario). MCT is the developer of the PLCOm2012 lung cancer risk prediction model. Use of the model is free of charge to all non-commercial users of the PLCOm2012, whether clinical or personal use. MCT has assigned the commercial intellectual property rights to Brock University. Part of the net proceeds from Brock University’s commercial licensing of use of the PLCOm2012 is to be paid to MCT. To date no such payments have been made to or received by MCT. At Cancer Care Ontario, MCT is Senior Scientist and Scientific Lead for the High Risk Lung Cancer Screening Pilot Studies, which plan to begin recruitment in April 2017. Recruitment will be based on lung cancer risk estimated by the PLCOm2012. Cancer Care Ontario is the agency representing Ontario’s Ministry of Health and Long-Term Care for cancer screening and is a not-for-profit organization. Neither Cancer Care Ontario nor MCT will receive any funds for use of the PLCOm2012 in the pilot studies or subsequently if lung cancer screening of high-risk individuals is expanded across Ontario. MCT was an invited speaker at the following meetings in which the PLCOm2012 model was discussed and MCT travel expenses were in part paid for. In none of these presentations did the total expenses paid for exceed the actual total costs, i.e., MCT did not financially benefit from the presentation. 1. MCT, Invited speaker: Selection Criteria for Lung Cancer Screening – Incidence versus Mortality Models. Cancer Intervention and Surveillance Modeling Network (CISNET) meeting, Ann Arbor, Michigan, 6 May 2013. 2. MCT, Invited speaker: Modeling Lung Cancer Risk, In Symposium: Lung Cancer Screening: Moving Forward, and Looking Forward. American Thoracic Society (ATS) Annual Meeting. May 17-22, 2013, Philadelphia, Pennsylvania. 3. MCT, Invited speaker: Lung Cancer Screening, In Symposium: High-Risk Populations and Cancer Screening. American Society for Clinical Oncology (ASCO) Annual Meeting. June 1-4, 2013, Chicago, Illinois. 4. MCT, Invited speaker: Risk Stratification for Lung Cancer Screening Studies. In session: Low-dose computed lung screening. At the 15th International Association for the Study of Lung Cancer (IASLC) World Conference on Lung Cancer. October 28, 2013, Sydney, Australia. 5. MCT, Invited speaker: Screening for lung cancer. At the Canadian Lung Cancer Conference. 7 February 2014, Vancouver, BC. 6. MCT, Invited speaker: Lung Cancer Screening – Issues & Updates. 9th Ontario Thoracic Cancer Conference. Niagara-on-the-Lake. 26 April 2014. 7. MCT, Invited speaker: Risk models for selection of individuals for lung cancer screening. Pan-Canadian Lung Cancer Screening Meeting Montreal, QC. 29 May 2014. 8. MCT, Invited speaker: Lung cancer risk models for targeting screening. Cancer Intervention and Surveillance Modeling Network (CISNET) meeting. Minneapolis, MN. June 2, 2014. 9. MCT, Invited speaker: Selection of Individuals for Lung Cancer Screening. McMaster University – Juravinski Cancer Center – Regional Oncology Rounds. Hamilton, ON. 13 November 2014. 10. MCT, Invited speaker: Lung cancer risk and screening. Cancer Intervention and Surveillance Modeling Network (CISNET) annual meeting. Bethesda, MD. December 10, 2014. 11. MCT, Invited speaker: National Academy of Sciences, Institute of Medicine, National Cancer Policy Forum, Workshop – Implementation of Lung Cancer Screening. Identifying High-Risk Populations for Screening: Risk Modeling – Current Ideas, New Developments, and Future Potentials. June 20-21, 2016, Washington, D.C.
Figures
Comment in
-
Selecting high-risk individuals for lung cancer screening; the use of risk prediction models vs. simplified eligibility criteria.Ann Transl Med. 2017 Oct;5(20):406. doi: 10.21037/atm.2017.07.14. Ann Transl Med. 2017. PMID: 29152506 Free PMC article. No abstract available.
References
-
- Humphrey LL, Deffebach M, Pappas M, Baumann C, Artis K, Mitchell JP, et al. Screening for lung cancer with low-dose computed tomography: a systematic review to update the US Preventive services task force recommendation. Ann Intern Med. 2013;159(6):411–20. 10.7326/0003-4819-159-6-201309170-00690 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
