

Local Treatment of Unresectable Colorectal Liver Metastases: Results of a Randomized Phase II Trial
- PMID: 28376151
- PMCID: PMC5408999
- DOI: 10.1093/jnci/djx015
Local Treatment of Unresectable Colorectal Liver Metastases: Results of a Randomized Phase II Trial
Abstract
Background: Tumor ablation is often employed for unresectable colorectal liver metastases. However, no survival benefit has ever been demonstrated in prospective randomized studies. Here, we investigate the long-term benefits of such an aggressive approach.
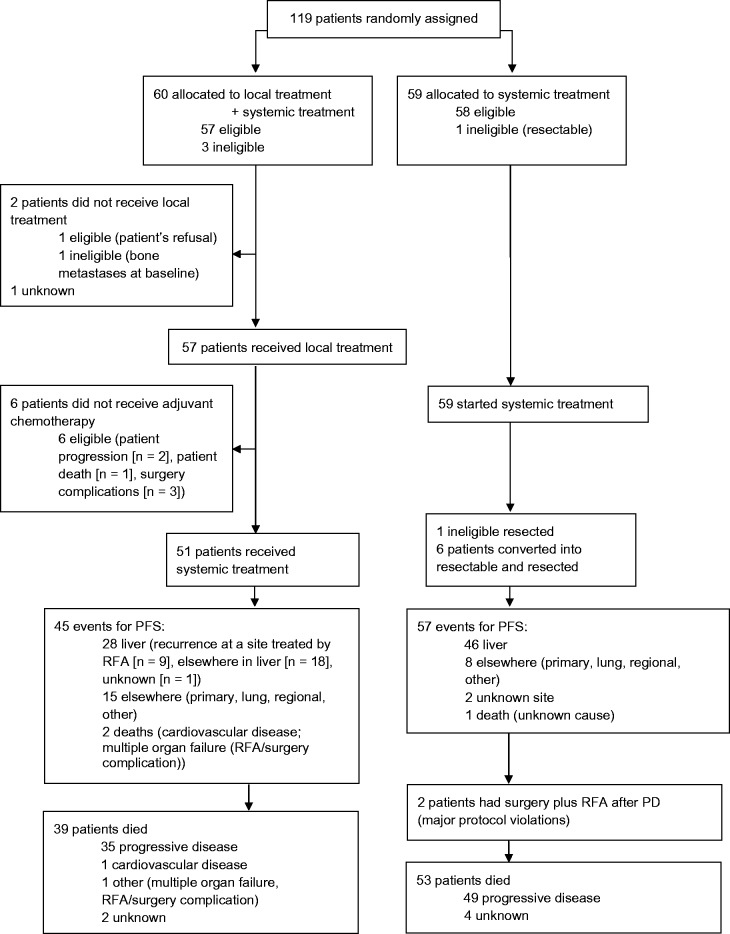
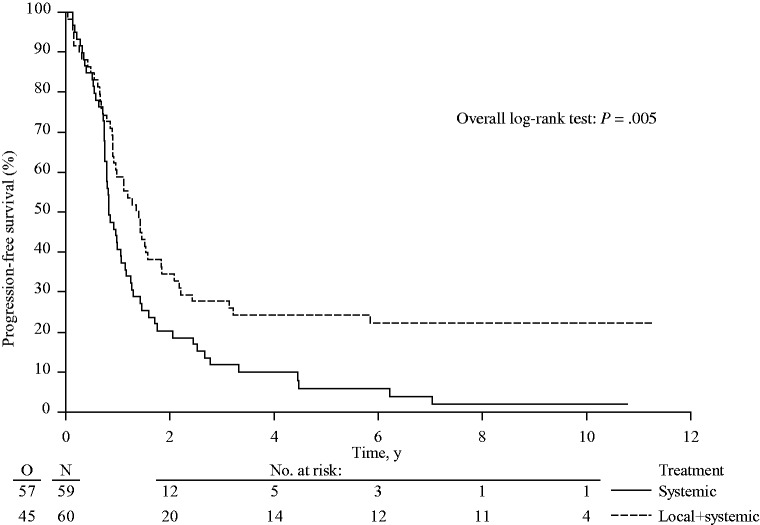
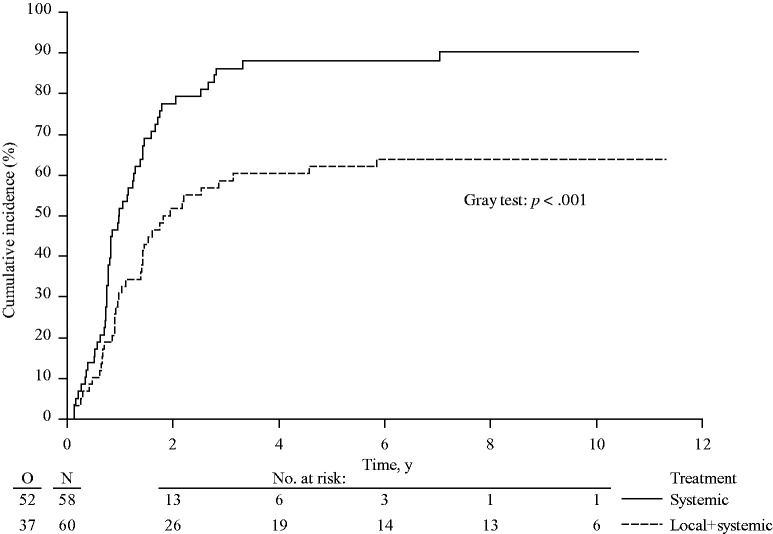
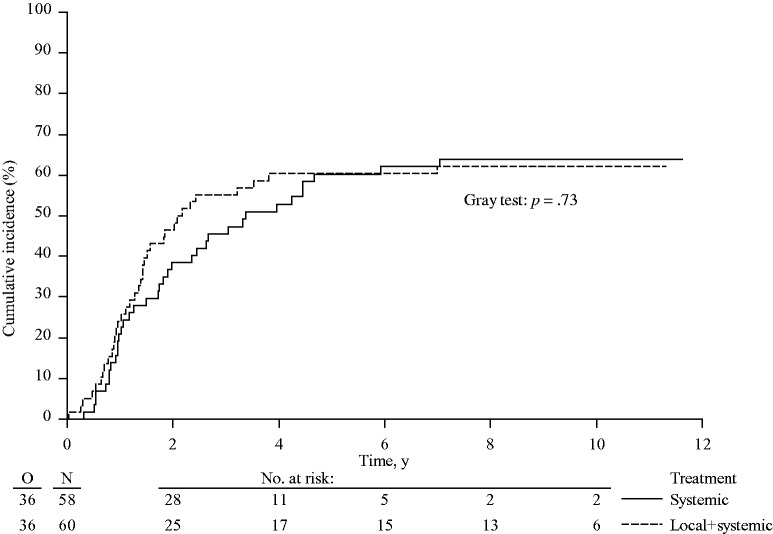
Methods: In this randomized phase II trial, 119 patients with unresectable colorectal liver metastases (n < 10 and no extrahepatic disease) received systemic treatment alone or systemic treatment plus aggressive local treatment by radiofrequency ablation ± resection. Previously, we reported that the primary end point (30-month overall survival [OS] > 38%) was met. We now report on long-term OS results. All statistical tests were two-sided. The analyses were according to intention to treat.
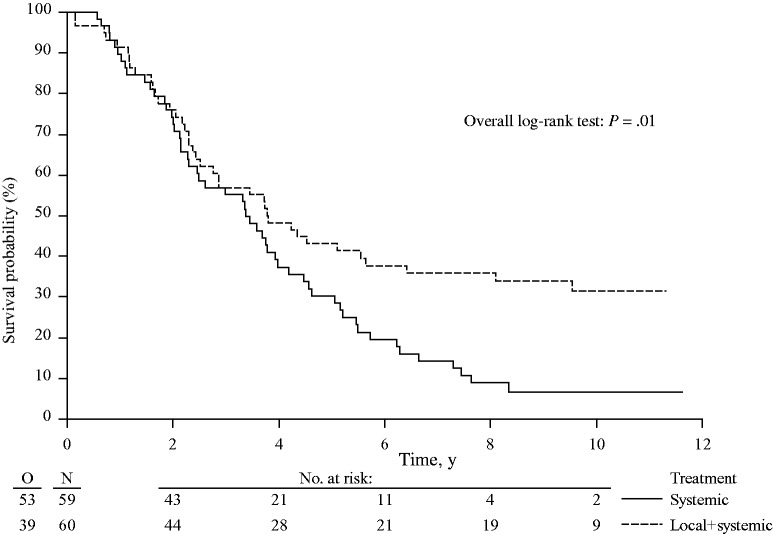
Results: At a median follow up of 9.7 years, 92 of 119 (77.3%) patients had died: 39 of 60 (65.0%) in the combined modality arm and 53 of 59 (89.8%) in the systemic treatment arm. Almost all patients died of progressive disease (35 patients in the combined modality arm, 49 patients in the systemic treatment arm). There was a statistically significant difference in OS in favor of the combined modality arm (hazard ratio [HR] = 0.58, 95% confidence interval [CI] = 0.38 to 0.88, P = .01). Three-, five-, and eight-year OS were 56.9% (95% CI = 43.3% to 68.5%), 43.1% (95% CI = 30.3% to 55.3%), 35.9% (95% CI = 23.8% to 48.2%), respectively, in the combined modality arm and 55.2% (95% CI = 41.6% to 66.9%), 30.3% (95% CI = 19.0% to 42.4%), 8.9% (95% CI = 3.3% to 18.1%), respectively, in the systemic treatment arm. Median OS was 45.6 months (95% CI = 30.3 to 67.8 months) in the combined modality arm vs 40.5 months (95% CI = 27.5 to 47.7 months) in the systemic treatment arm.
Conclusions: This phase II trial is the first randomized study demonstrating that aggressive local treatment can prolong OS in patients with unresectable colorectal liver metastases.
© The Author 2017. Published by Oxford University Press.
Figures
Comment in
-
Local Therapy for Colorectal Liver Metastases: Establishing Today's Level of Evidence and Defining Tomorrow's Roadmap.J Natl Cancer Inst. 2017 Sep 1;109(9). doi: 10.1093/jnci/djx018. J Natl Cancer Inst. 2017. PMID: 28376150 No abstract available.
-
[Unresectable colorectal liver metastases : Prolonged survival with aggressive local therapy].Chirurg. 2017 Sep;88(9):803. doi: 10.1007/s00104-017-0486-0. Chirurg. 2017. PMID: 28741171 German. No abstract available.
-
RE: Local Treatment of Unresectable Colorectal Liver Metastases: Results of a Randomized Phase II Trial.J Natl Cancer Inst. 2017 Oct 1;109(10). doi: 10.1093/jnci/djx149. J Natl Cancer Inst. 2017. PMID: 29117361 No abstract available.
References
-
- House MG, Ito H, Gönen M, et al. Survival after hepatic resection for metastatic colorectal cancer: Trends in outcomes for 1,600 patients during two decades at a single institution. J Am Coll Surg. 2010;210(5):744–752, 752–755. - PubMed
-
- Nordlinger B, Sorbye H, Glimelius B, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable livermetastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14(12):1208–1215. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
