

Evaluation of Polygenic Risk Scores for Breast and Ovarian Cancer Risk Prediction in BRCA1 and BRCA2 Mutation Carriers
- PMID: 28376175
- PMCID: PMC5408990
- DOI: 10.1093/jnci/djw302
Evaluation of Polygenic Risk Scores for Breast and Ovarian Cancer Risk Prediction in BRCA1 and BRCA2 Mutation Carriers
Abstract
Background: Genome-wide association studies (GWAS) have identified 94 common single-nucleotide polymorphisms (SNPs) associated with breast cancer (BC) risk and 18 associated with ovarian cancer (OC) risk. Several of these are also associated with risk of BC or OC for women who carry a pathogenic mutation in the high-risk BC and OC genes BRCA1 or BRCA2. The combined effects of these variants on BC or OC risk for BRCA1 and BRCA2 mutation carriers have not yet been assessed while their clinical management could benefit from improved personalized risk estimates.
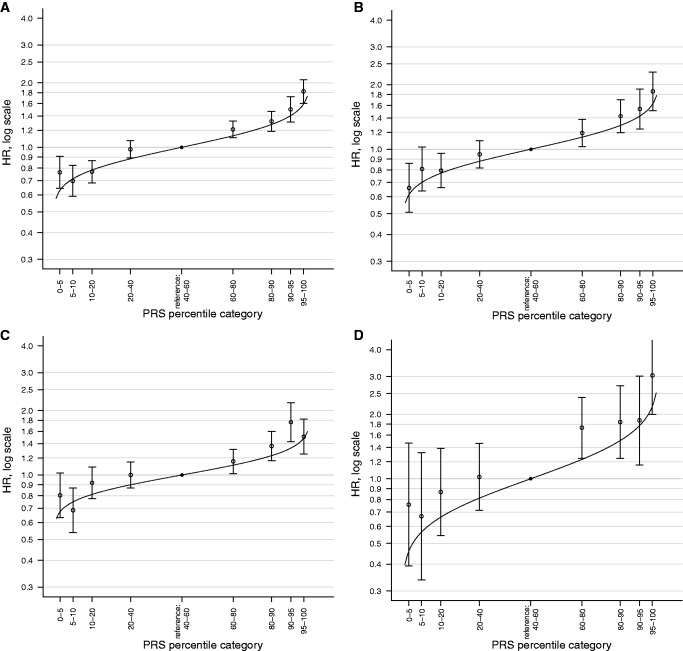
Methods: We constructed polygenic risk scores (PRS) using BC and OC susceptibility SNPs identified through population-based GWAS: for BC (overall, estrogen receptor [ER]-positive, and ER-negative) and for OC. Using data from 15 252 female BRCA1 and 8211 BRCA2 carriers, the association of each PRS with BC or OC risk was evaluated using a weighted cohort approach, with time to diagnosis as the outcome and estimation of the hazard ratios (HRs) per standard deviation increase in the PRS.
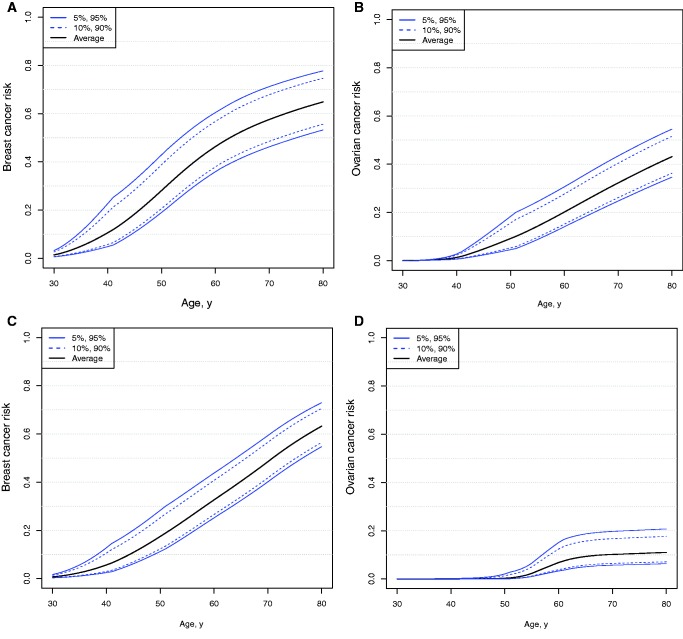
Results: The PRS for ER-negative BC displayed the strongest association with BC risk in BRCA1 carriers (HR = 1.27, 95% confidence interval [CI] = 1.23 to 1.31, P = 8.2×10 -53 ). In BRCA2 carriers, the strongest association with BC risk was seen for the overall BC PRS (HR = 1.22, 95% CI = 1.17 to 1.28, P = 7.2×10 -20 ). The OC PRS was strongly associated with OC risk for both BRCA1 and BRCA2 carriers. These translate to differences in absolute risks (more than 10% in each case) between the top and bottom deciles of the PRS distribution; for example, the OC risk was 6% by age 80 years for BRCA2 carriers at the 10th percentile of the OC PRS compared with 19% risk for those at the 90th percentile of PRS.
Conclusions: BC and OC PRS are predictive of cancer risk in BRCA1 and BRCA2 carriers. Incorporation of the PRS into risk prediction models has promise to better inform decisions on cancer risk management.
© The Author 2017. Published by Oxford University Press.
Figures
References
-
- Evans DG, Graham J, O'Connell S, et al. Familial breast cancer: Summary of updated NICE guidance. BMJ. 2013;346:f3829. - PubMed
-
- Clark AS, Domchek SM. Clinical management of hereditary breast cancer syndromes. J Mammary Gland Biol Neoplasia. 2011;16(1):17–25. - PubMed
-
- Parker WH, Jacoby V, Shoupe D, et al. Effect of bilateral oophorectomy on women's long-term health. Womens Health (Lond Engl). 2009;5(5):565–576. - PubMed
MeSH terms
Substances
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- UG1 CA189867/CA/NCI NIH HHS/United States
- 20861/CRUK_/Cancer Research UK/United Kingdom
- U01 CA116167/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- P50 CA116201/CA/NCI NIH HHS/United States
- 15007/CRUK_/Cancer Research UK/United Kingdom
- 10118/CRUK_/Cancer Research UK/United Kingdom
- R01 CA176785/CA/NCI NIH HHS/United States
- 17528/CRUK_/Cancer Research UK/United Kingdom
- 16561/CRUK_/Cancer Research UK/United Kingdom
- 23382/CRUK_/Cancer Research UK/United Kingdom
- 10124/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
