

Breast Cancer Risk and Progressive Histology in Serial Benign Biopsies
- PMID: 28376198
- PMCID: PMC5412118
- DOI: 10.1093/jnci/djx035
Breast Cancer Risk and Progressive Histology in Serial Benign Biopsies
Abstract
Background: More than 1 million women per year in the United States with benign breast biopsies are known to be at elevated risk for breast cancer (BC), with risk stratified on histologic categories of epithelial proliferation. Here we assessed women who had serial benign biopsies over time and how changes in the histologic classification affected BC risk.
Methods: In the Mayo Clinic Benign Breast Disease Cohort of 13 466 women, 1414 women had multiple metachronous benign biopsies (10.5%). Both initial and subsequent biopsies were assessed histologically. BC risk for clinical and prognostic factors was assessed using subdistribution models to account for competing risks, and logistic regression/Wilcoxon/chi-square tests to assess covariates. All statistical tests were two-sided.
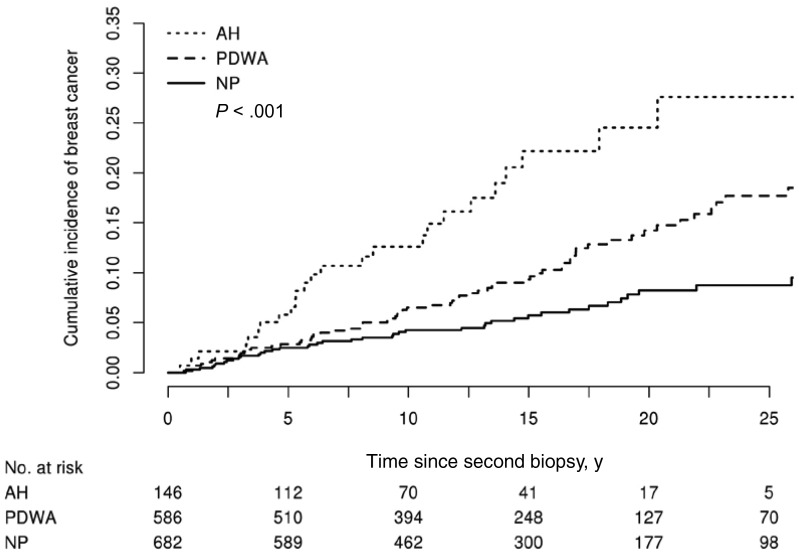
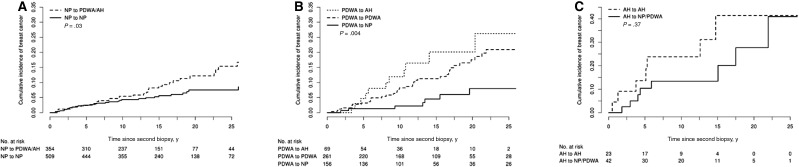
Results: Breast cancer risk for women with serial biopsies, stratified by histologic category in the later biopsies, was similar to women with a single biopsy. We found that changes in histological category between initial and subsequent biopsy statistically significantly impacted BC risk. Women with nonproliferative initial findings and subsequent proliferative findings had an increased risk (hazard ratio [HR] = 1.77, 95% confidence interval [CI] = 1.06 to 2.94, P = .03) compared with no change. Among women with proliferative disease without atypia at initial biopsy, risk decreased if later biopsy regressed to nonproliferative (HR = 0.49, 95% CI = 0.25 to 0.98) and increased if later biopsy showed progression to atypical hyperplasia (HR = 1.49, 95% CI = 0.73 to 3.05) compared with no change ( P = .04).
Conclusions: We found that breast cancer risk increases in women with progressive epithelial proliferation over time and decreases in women whose biopsies show less proliferation. This finding has important implications for effective clinical management of the 100 000 women per year who have multiple benign breast biopsies.
© The Author 2017. Published by Oxford University Press.
Figures
Comment in
-
Refining Risk Assessment in Women With Benign Breast Disease: An Ongoing Dilemma.J Natl Cancer Inst. 2017 Oct 1;109(10). doi: 10.1093/jnci/djx036. J Natl Cancer Inst. 2017. PMID: 28376199 No abstract available.
Similar articles
-
Multiplicity of benign breast lesions is a risk factor for progression to breast cancer.Clin Cancer Res. 2007 Sep 15;13(18 Pt 1):5474-9. doi: 10.1158/1078-0432.CCR-07-0928. Clin Cancer Res. 2007. PMID: 17875777
-
Effects of mammographic density and benign breast disease on breast cancer risk (United States).Cancer Causes Control. 2001 Feb;12(2):103-10. doi: 10.1023/a:1008935821885. Cancer Causes Control. 2001. PMID: 11246838
-
Flat epithelial atypia and risk of breast cancer: A Mayo cohort study.Cancer. 2015 May 15;121(10):1548-55. doi: 10.1002/cncr.29243. Epub 2015 Jan 13. Cancer. 2015. PMID: 25639678 Free PMC article.
-
Benign breast disease and cancer risk.Crit Rev Oncol Hematol. 1993 Dec;15(3):221-42. doi: 10.1016/1040-8428(93)90043-4. Crit Rev Oncol Hematol. 1993. PMID: 8142058 Review. No abstract available.
-
Clinical and histologic aspects of proliferative and non-proliferative benign breast disease.J Cell Biochem Suppl. 1993;17G:45-8. doi: 10.1002/jcb.240531108. J Cell Biochem Suppl. 1993. PMID: 8007708 Review.
Cited by
-
Breast biopsies and breast cancer risk in Israeli BRCA germline pathogenic variant carriers.Breast Cancer Res Treat. 2025 Oct;213(3):377-384. doi: 10.1007/s10549-025-07787-3. Epub 2025 Jul 22. Breast Cancer Res Treat. 2025. PMID: 40694193 Free PMC article.
-
Association of SNP rs5069 in APOA1 with Benign Breast Diseases in a Mexican Population.Genes (Basel). 2022 Apr 22;13(5):738. doi: 10.3390/genes13050738. Genes (Basel). 2022. PMID: 35627123 Free PMC article.
-
Analysis of Lifestyle and Genetic Risk Factors in Urban Women in China Who Had Malignant or Suspected Malignant Breast Nodules Identified via Breast Cancer Screening.Breast Care (Basel). 2025 Mar 21:1-13. doi: 10.1159/000545279. Online ahead of print. Breast Care (Basel). 2025. PMID: 40331129 Free PMC article.
-
Therapeutic Effects of a Traditional Chinese Medicine Formula Plus Tamoxifen vs. Tamoxifen for the Treatment of Mammary Gland Hyperplasia: A Meta-Analysis of Randomized Trials.Front Pharmacol. 2018 Feb 2;9:45. doi: 10.3389/fphar.2018.00045. eCollection 2018. Front Pharmacol. 2018. PMID: 29456506 Free PMC article. Review.
-
High-resolution microCT to assess breast microcalcification morphometry by histologic lesion subtype and radiologic classification.Breast Cancer Res Treat. 2025 Nov;214(1):49-58. doi: 10.1007/s10549-025-07792-6. Epub 2025 Aug 17. Breast Cancer Res Treat. 2025. PMID: 40819343
References
-
- Gutwein LG, Ang DN, Liu H, et al. Utilization of minimally invasive breast biopsy for the evaluation of suspicious breast lesions. Am J Surg. 2011;202:127–132. - PubMed
-
- Silverstein M. Where's the outrage? J Am Coll Surg. 2009;208:78–79. - PubMed
-
- Dupont WD, Parl FF, Hartmann WH, et al. Breast cancer risk associated with proliferative breast disease and atypical hyperplasia. Cancer. 1993;71:1258–1265. - PubMed
-
- Hartmann LC, Sellers TA, Frost MH, et al. Benign breast disease and the risk of breast cancer. N Engl J Med. 2005;353:229–237. - PubMed
-
- McDivitt RW, Stevens JA, Lee NC, Wingo PA, Rubin GL, Gersell D.. Histologic types of benign breast disease and the risk for breast cancer. The Cancer and Steroid Hormone Study Group. Cancer. 1992;69:1408–1414. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
