

Peer Support Interventions for Adults With Diabetes: A Meta-Analysis of Hemoglobin A1c Outcomes
- PMID: 28376441
- PMCID: PMC5389404
- DOI: 10.1370/afm.1982
Peer Support Interventions for Adults With Diabetes: A Meta-Analysis of Hemoglobin A1c Outcomes
Abstract
Purpose: Peer support intervention trials have shown varying effects on glycemic control. We aimed to estimate the effect of peer support interventions delivered by people affected by diabetes (those with the disease or a caregiver) on hemoglobin A1c (HbA1c) levels in adults.
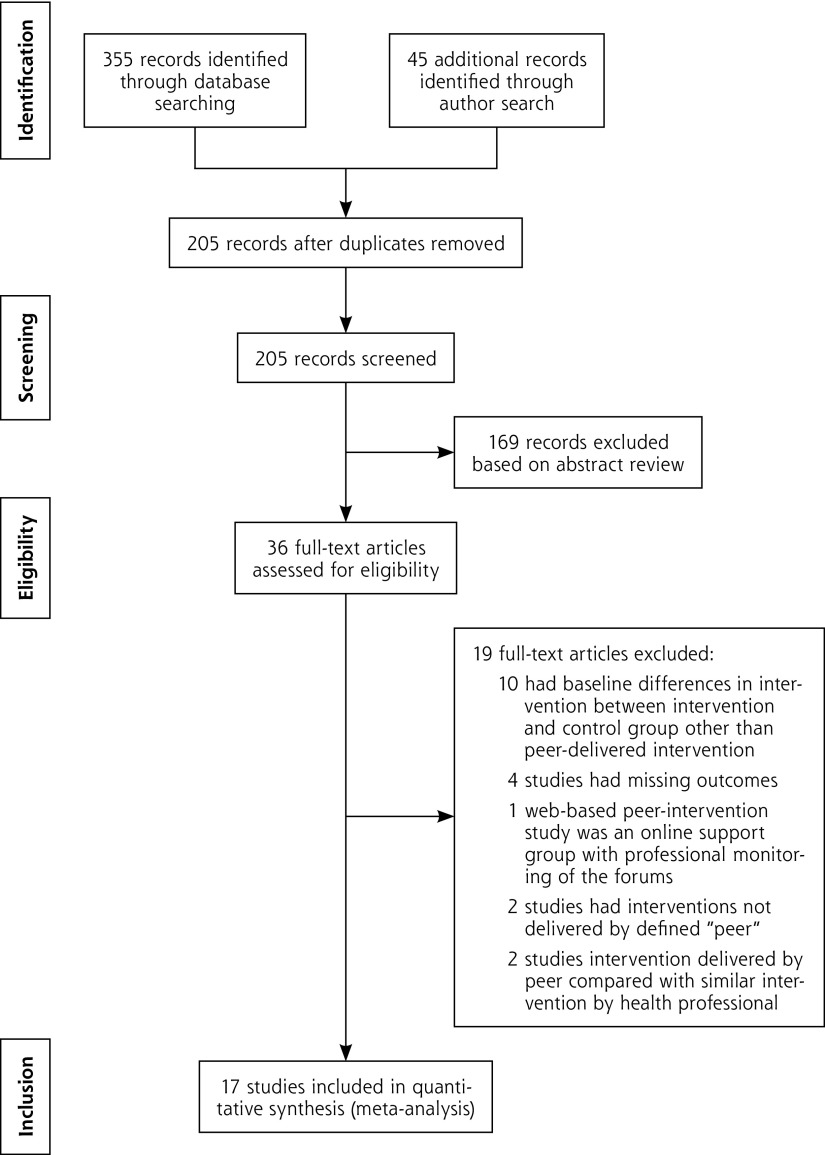
Methods: We searched multiple databases from 1960 to November 2015, including Ovid MEDLINE, the Cochrane Central Register of Controlled Trials, CINAHL, and Scopus. We included randomized controlled trials (RCTs) of adults with diabetes receiving peer support interventions compared with otherwise similar care. Seventeen of 205 retrieved studies were eligible for inclusion. Quality was assessed with the Cochrane risk of bias tool. We calculated the standardized mean difference (SMD) of change in HbA1c level from baseline between groups using a random effects model. Subgroup analyses were predefined.
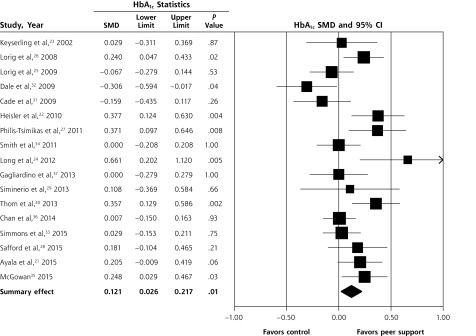
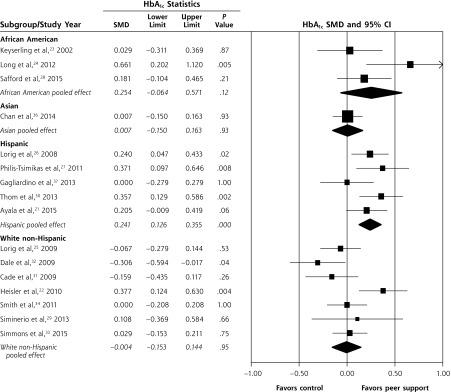
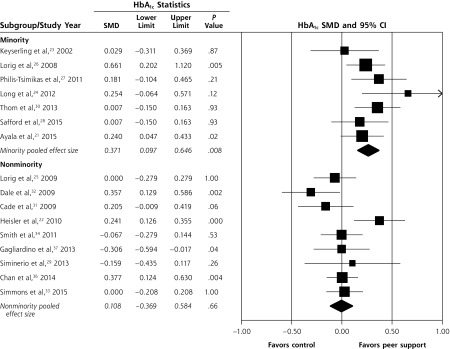
Results: Seventeen studies (3 cluster RCTs, 14 RCTs) with 4,715 participants showed an improvement in pooled HbA1c level with an SMD of 0.121 (95% CI, 0.026-0.217; P = .01; I2 = 60.66%) in the peer support intervention group compared with the control group; this difference translated to an improvement in HbA1c level of 0.24% (95% CI, 0.05%-0.43%). Peer support interventions showed an HbA1c improvement of 0.48% (95% CI, 0.25%-0.70%; P <.001; I2 = 17.12%) in the subset of studies with predominantly Hispanic participants and 0.53% (95% CI, 0.32%-0.73%; P <.001; I2 = 9.24%) in the subset of studies with predominantly minority participants; both were clinically relevant. In sensitivity analysis excluding cluster RCTs, the overall effect size changed little.
Conclusions: Peer support interventions for diabetes overall achieved a statistically significant but minor improvement in HbA1c levels. These interventions may, however, be particularly effective in improving glycemic control for people from minority groups, especially those of Hispanic ethnicity.
Keywords: diabetes mellitus; glycemic control; hemoglobin A1c; peer support; self-efficacy; support groups.
© 2016 Annals of Family Medicine, Inc.
Figures
References
-
- Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103(2):137–149. - PubMed
-
- Strawbridge LM, Lloyd JT, Meadow A, Riley GF, Howell BL. Use of Medicare’s diabetes self-management training benefit. Health Educ Behav. 2015;42(4):530–538. - PubMed
-
- Duncan I, Ahmed T, Li QE, et al. Assessing the value of the diabetes educator. Diabetes Educ. 2011;37(5):638–657. - PubMed
-
- Li R, Shrestha SS, Lipman R, Burrows NR, Kolb LE, Rutledge S; Centers for Disease Control and Prevention (CDC). Diabetes self-management education and training among privately insured persons with newly diagnosed diabetes—United States, 2011–2012. MMWR Morb Mortal Wkly Rep. 2014;63(46):1045–1049. - PMC - PubMed
-
- Norris SL, Lau J, Smith SJ, Schmid CH, Engelgau MM. Self-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care. 2002;25(7):1159–1171. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous