

Health Benefits and Cost-Effectiveness of Brief Clinician Tobacco Counseling for Youth and Adults
- PMID: 28376459
- PMCID: PMC5217842
- DOI: 10.1370/afm.2022
Health Benefits and Cost-Effectiveness of Brief Clinician Tobacco Counseling for Youth and Adults
Abstract
Purpose: To help clinicians and care systems determine the priority for tobacco counseling in busy clinic schedules, we assessed the lifetime health and economic value of annually counseling youth to discourage smoking initiation and of annually counseling adults to encourage cessation.
Methods: We conducted a microsimulation analysis to estimate the health impact and cost effectiveness of both types of tobacco counseling in a US birth cohort of 4,000,000. The model used for the analysis was constructed from nationally representative data sets and structured literature reviews.
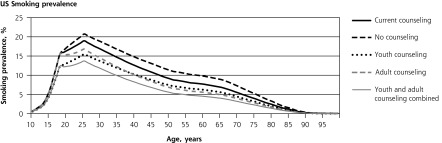
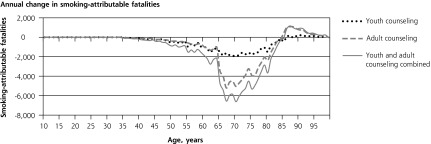
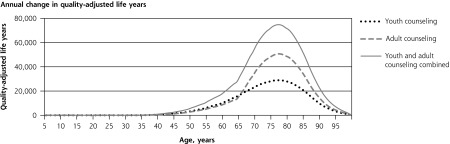
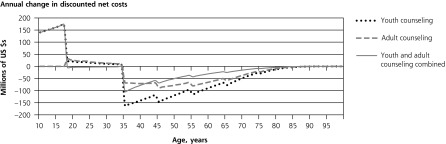
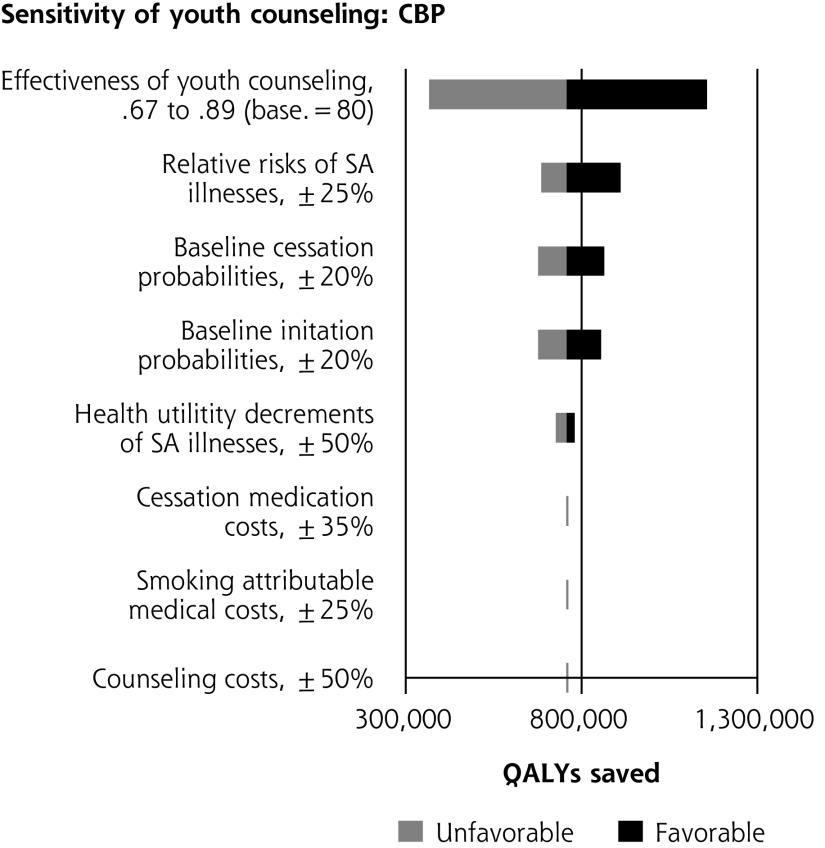
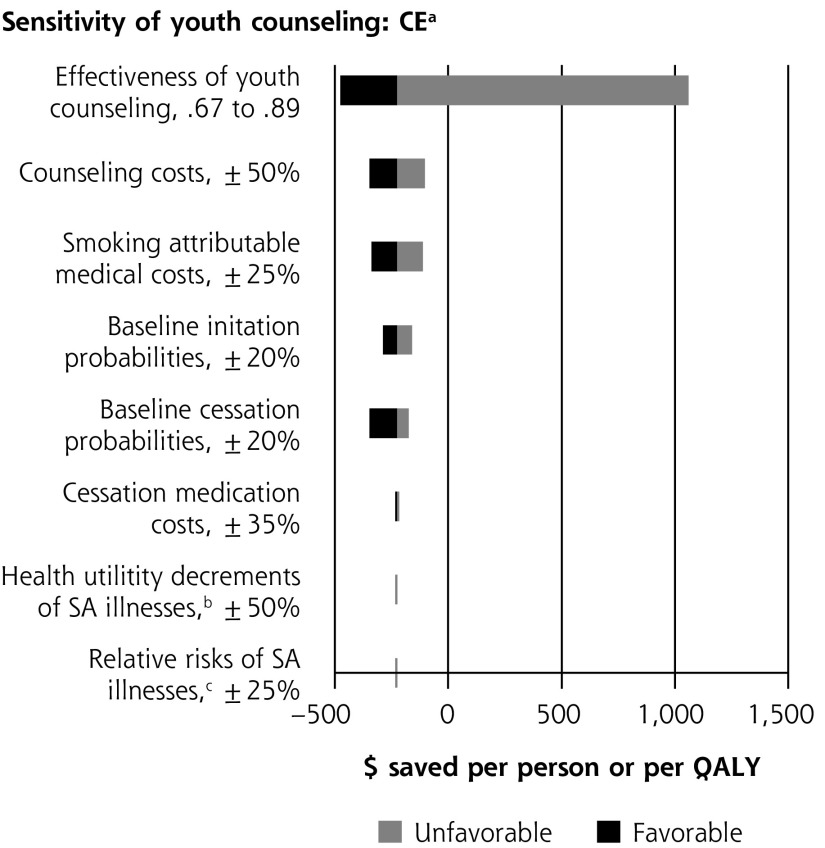
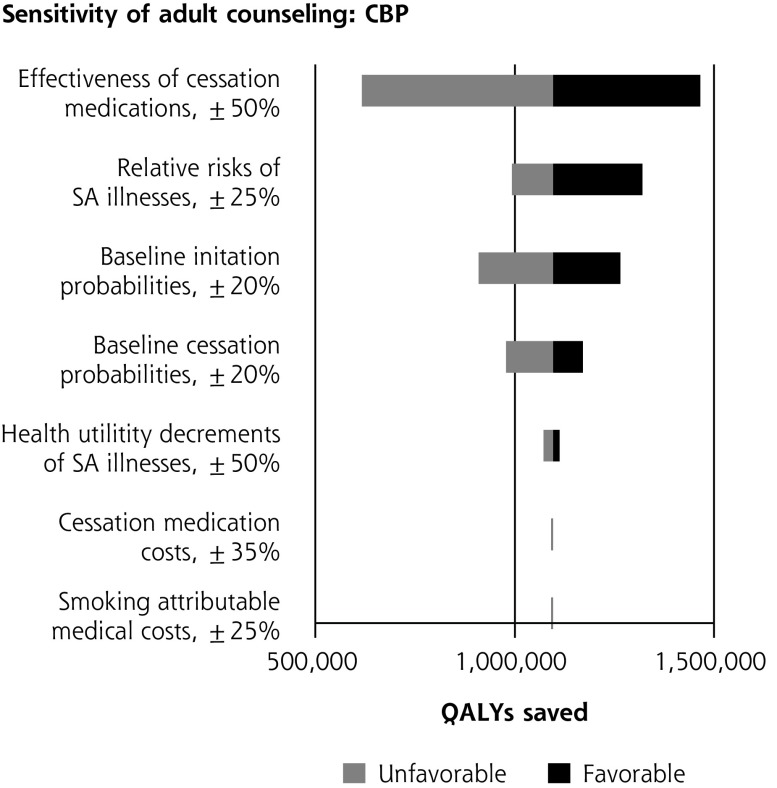
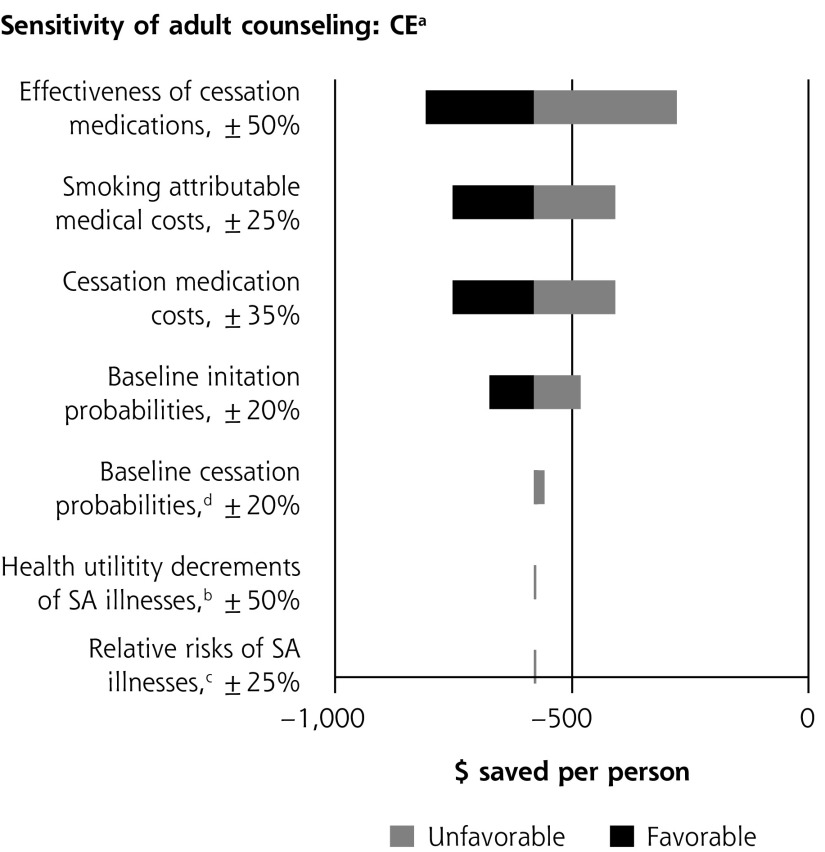
Results: Compared with no tobacco counseling, the model predicts that annual counseling for youth would reduce the average prevalence of smoking cigarettes during adult years by 2.0 percentage points, whereas annual counseling for adults will reduce prevalence by 3.8 percentage points. Youth counseling would prevent 42,686 smoking-attributable fatalities and increase quality-adjusted life years (QALYs) by 756,601 over the lifetime of the cohort. Adult counseling would prevent 69,901 smoking-attributable fatalities and increase QALYs by 1,044,392. Youth and adult counseling would yield net savings of $225 and $580 per person, respectively. If annual tobacco counseling was provided to the cohort during both youth and adult years, then adult smoking prevalence would be 5.5 percentage points lower compared with no counseling, and there would be 105,917 fewer smoking-attributable fatalities over their lifetimes. Only one-third of the potential health and economic benefits of counseling are being realized at current counseling rates.
Conclusions: Brief tobacco counseling provides substantial health benefits while producing cost savings. Both youth and adult intervention are high-priority uses of limited clinician time.
Keywords: cigarette smoking; cost-effectiveness; counseling; health impact; prioritization; tobacco.
© 2017 Annals of Family Medicine, Inc.
Conflict of interest statement
Conflicts of interest: authors report none.
Figures
Comment in
-
Strategies to Prioritize Clinical Options in Primary Care.Ann Fam Med. 2017 Jan;15(1):10-13. doi: 10.1370/afm.2027. Epub 2017 Jan 6. Ann Fam Med. 2017. PMID: 28376456 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention. Early Release of Selected Estimates Based on Data From the National Health Interview Survey, 2015. https://www.cdc.gov/nchs/data/nhis/earlyrelease/earlyrelease201605_08.pdf. Published 2016.
-
- US Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General, 2014. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
-
- Singh T, Arrazola RA, Corey CG, et al. Tobacco use among middle and high school students—United States, 2011–2015. MMWR Morb Mortal Wkly Rep. 2016;65(14):361–367. - PubMed
-
- Siu AL; U.S. Preventive Services Task Force. Behavioral and pharmacotherapy interventions for tobacco smoking cessation in adults, including pregnant women: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163(8):622–634. - PubMed
-
- Patnode CD, Henderson JT, Thompson JH, Senger CA, Fortmann SP, Whitlock EP. Behavioral counseling and pharmacotherapy interventions for tobacco cessation in adults, including pregnant women: a review of reviews for the U.S. Preventive Services Task Force. Ann Intern Med. 2015;163(8):608–621. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources