

Volume and Characteristics of Intracerebral Hemorrhage with Direct Oral Anticoagulants in Comparison with Warfarin
- PMID: 28376486
- PMCID: PMC5425761
- DOI: 10.1159/000462985
Volume and Characteristics of Intracerebral Hemorrhage with Direct Oral Anticoagulants in Comparison with Warfarin
Abstract
Background: Patients undergoing anticoagulation therapy often experience intracerebral hemorrhages (ICHs), and warfarin in particular is known to increase hematoma expansion in ICHs, which results in a poor outcome. Recent studies reported that, in comparison with warfarin, direct oral anticoagulants (DOACs) cause fewer ICHs with better functional outcome. However, since it is still unknown whether DOACs are associated with a smaller hematoma volume of ICHs, we aimed to compare the volume, hematoma expansion, and outcomes associated with ICHs treated with DOACs and warfarin.
Methods: We performed a prospective multicenter cross-sectional study. The subjects included patients with acute ICHs who received either DOACs or warfarin. We evaluated the clinical characteristics, and measured initial and follow-up ICH volumes. The volume of ICHs and hematoma expansion were compared between the DOAC and warfarin groups. Mortality and modified Rankin score at discharge were evaluated as outcomes.
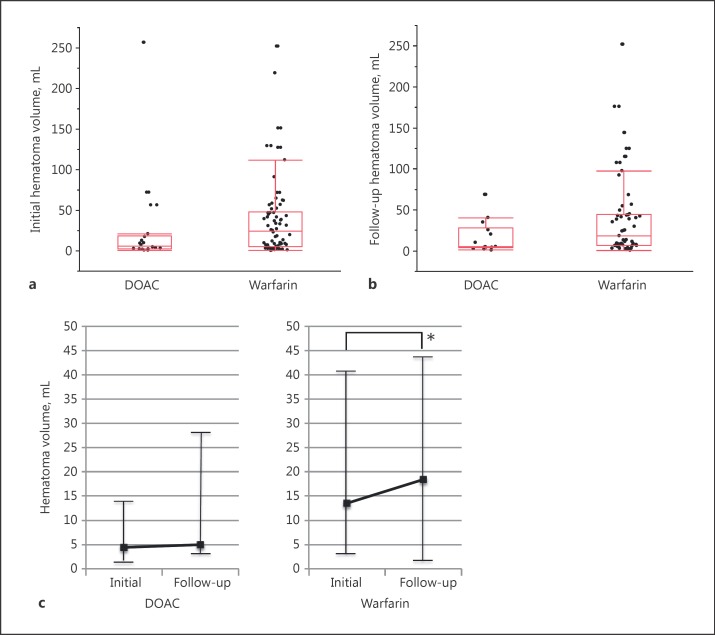
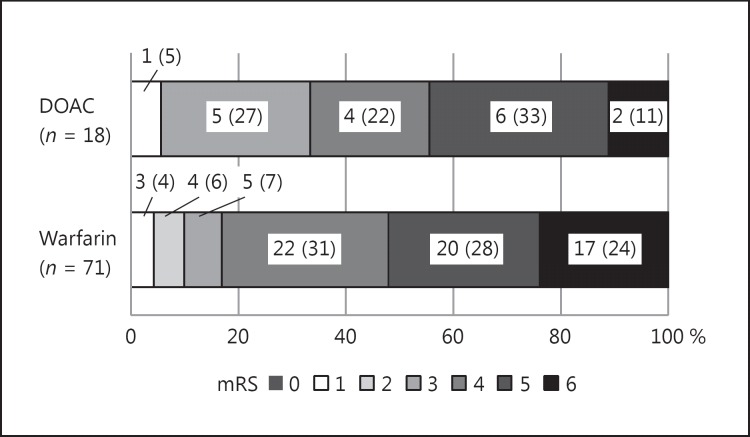
Results: There were 18 patients in the DOAC group and 71 in the warfarin group. The baseline characteristics were similar between the 2 groups. Initial median hematoma volume of ICHs in the DOAC group was significantly lower than that in the warfarin group (6.2 vs. 24.2 mL, respectively; p = 0.04). In cases involving follow-up computed tomography scanning, the median hematoma volume of ICHs at follow-up was lower in the DOAC group than in the warfarin group (initial: DOACs 4.4 vs. warfarin 13.5 mL; follow-up: 5.0 vs. 18.4 mL, respectively; p = 0.05). Further, the hematoma in ICHs associated with DOACs did not expand. Although the mortality of ICHs associated with DOACs (11%) was lower than that associated with warfarin (24%), this difference was not statistically significant. The univariate analysis showed that the anticoagulant type (DOACs vs. warfarin) and sex (male vs. female) were associated with ICH volume. The multivariable linear regression showed that the use of DOACs (compared to warfarin; β: -0.23, p = 0.03) and female sex (compared to male; β: -0.25, p = 0.02) were associated with a small hematoma volume.
Conclusions: Based on the results of the present study, in terms of the risks associated with ICHs, the use of DOACs appears to be safer than warfarin for anticoagulation therapy. Further studies are required to validate these findings. .
Keywords: Anticoagulants; Hemorrhage associated with oral anticoagulation; Intracerebral hemorrhage.
© 2017 The Author(s) . Published by S. Karger AG, Basel.
Figures
References
-
- Flibotte JJ, Hagan N, O'Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology. 2004;63:1059–1064. - PubMed
-
- Toyoda K, Yasaka M, Iwade K, Nagata K, Koretsune Y, Sakamoto T, et al. Dual antithrombotic therapy increases severe bleeding events in patients with stroke and cardiovascular disease: a prospective, multicenter, observational study. Stroke. 2008;39:1740–1745. - PubMed
-
- Kuwashiro T, Yasaka M, Itabashi R, Nakagaki H, Miyashita F, Naritomi H, et al. Enlargement of acute intracerebral hematomas in patients on long-term warfarin treatment. Cerebrovasc Dis. 2010;29:446–453. - PubMed
-
- Hankey GJ, Stevens SR, Piccini JP, Lokhnygina Y, Mahaffey KW, Halperin JL, et al. Intracranial hemorrhage among patients with atrial fibrillation anticoagulated with warfarin or rivaroxaban: the rivaroxaban once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation. Stroke. 2014;45:1304–1312. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
