

Fat in the lumbar multifidus muscles - predictive value and change following disc prosthesis surgery and multidisciplinary rehabilitation in patients with chronic low back pain and degenerative disc: 2-year follow-up of a randomized trial
- PMID: 28376754
- PMCID: PMC5381060
- DOI: 10.1186/s12891-017-1505-5
Fat in the lumbar multifidus muscles - predictive value and change following disc prosthesis surgery and multidisciplinary rehabilitation in patients with chronic low back pain and degenerative disc: 2-year follow-up of a randomized trial
Abstract
Background: Evidence is lacking on whether fat infiltration in the multifidus muscles affects outcomes after total disc replacement (TDR) surgery and if it develops after surgery. The aims of this study were 1) to investigate whether pre-treatment multifidus muscle fat infiltration predicts outcome 2 years after treatment with TDR surgery or multidisciplinary rehabilitation, and 2) to compare changes in multifidus muscle fat infiltration from pre-treatment to 2-year follow-up between the two treatment groups.
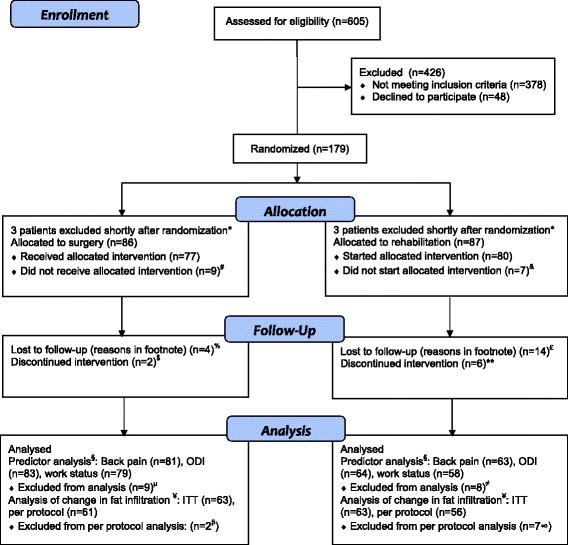
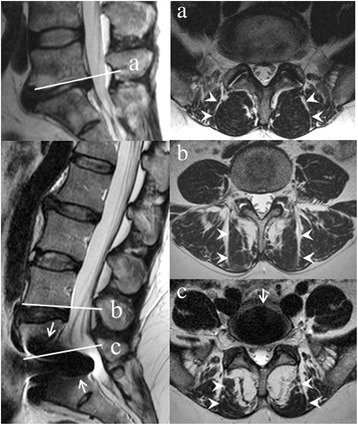
Methods: The study is secondary analysis of data from a trial with 2-year follow-up of patients with chronic low back pain (LBP) and degenerative disc randomized to TDR surgery or multidisciplinary rehabilitation. We analyzed (aim 1) patients with both magnetic resonance imaging (MRI) at pre-treatment and valid data on outcome measures at 2-year follow-up (predictor analysis), and (aim 2) patients with MRI at both pre-treatment and 2-year follow-up. Outcome measures were visual analogue scale (VAS) for LBP, Oswestry Disability Index (ODI), work status and muscle fat infiltration on MRI. Patients with pre-treatment MRI and 2-year outcome data on VAS for LBP (n = 144), ODI (n = 147), and work status (n = 137) were analyzed for prediction purposes. At 2-year follow-up, 126 patients had another MRI scan, and change in muscle fat infiltration was compared between the two treatment groups. Three radiologists visually quantified multifidus muscle fat in the three lower lumbar levels on MRI as <20% (grade 0), 20-50% (grade 1), or >50% (grade 2) of the muscle cross-section containing fat. Regression analysis and a mid-P exact test were carried out.
Results: Grade 0 pre-treatment multifidus muscle fat predicted better clinical results at 2-year follow-up after TDR surgery (all outcomes) but not after rehabilitation. At 2-year follow-up, increased fat infiltration was more common in the surgery group (intention-to-treat p = 0.03, per protocol p = 0.08) where it was related to worse pain and ODI.
Conclusions: Patients with less fat infiltration of multifidus muscles before TDR surgery had better outcomes at 2-year follow-up, but findings also indicated a negative influence of TDR surgery on back muscle morphology in some patients. The rehabilitation group maintained their muscular morphology and were unaffected by pre-treatment multifidus muscle fat.
Trial registration: NCT 00394732 (retrospectively registered October 31, 2006).
Trial registration: ClinicalTrials.gov NCT00394732.
Keywords: Change over time; Chronic degenerative low back pain; Multidisciplinary rehabilitation; Multifidus muscle fat; Physiotherapy; Predictive value; Surgery; Total disc replacement.
Figures
References
-
- Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J SpinalDisord. 1992;5(4):383–389. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
