

High pre-diagnosis attrition among patients with presumptive MDR-TB: an operational research from Bhopal district, India
- PMID: 28376789
- PMCID: PMC5379759
- DOI: 10.1186/s12913-017-2191-6
High pre-diagnosis attrition among patients with presumptive MDR-TB: an operational research from Bhopal district, India
Erratum in
-
Erratum to: High pre-diagnosis attrition among patients with presumptive MDR-TB: an operational research from Bhopal district, India.BMC Health Serv Res. 2017 Apr 24;17(1):301. doi: 10.1186/s12913-017-2252-x. BMC Health Serv Res. 2017. PMID: 28438143 Free PMC article. No abstract available.
Abstract
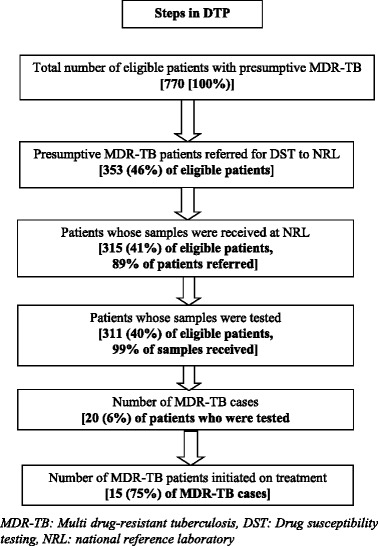
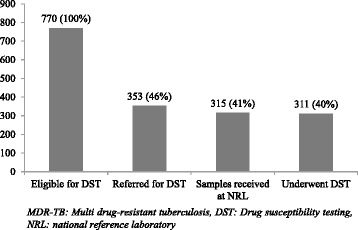
Background: Pre-diagnosis attrition needs to be addressed urgently if we are to make progress in improving MDR-TB case detection and achieve universal access to MDR-TB care. We report the pre-diagnosis attrition, along with factors associated, and turnaround times related to the diagnostic pathway among patient with presumptive MDR-TB in Bhopal district, central India (2014).
Methods: Study was conducted under the Revised National Tuberculosis Control Programme setting. It was a retrospective cohort study involving record review of all registered TB cases in Bhopal district that met the presumptive MDR-TB criteria (eligible for DST) in 2014. In quarter 1, Line Probe Assay (LPA) was used if sample was smear/culture positive. Quarter 2 onwards, LPA and Cartridge-based Nucleic Acid Amplification Test (CbNAAT) was used for smear positive and smear negative samples respectively. Pre-diagnosis attrition was defined as failure to undergo DST among patients with presumptive MDR-TB (as defined by the programme).
Results: Of 770 patients eligible for DST, 311 underwent DST and 20 patients were diagnosed as having MDR-TB. Pre-diagnosis attrition was 60% (459/770). Among those with pre-diagnosis attrition, 91% (417/459) were not identified as 'presumptive MDR-TB' by the programme. TAT [median (IQR)] to undergo DST after eligibility was 4 (0, 10) days. Attrition was more than 40% across all subgroups. Age more than 64 years; those from a medical college; those eligible in quarter 1; patients with presumptive criteria 'previously treated - recurrent TB', 'treatment after loss-to-follow-up' and 'previously treated-others'; and patients with extra-pulmonary TB were independent risk factors for not undergoing DST.
Conclusion: High pre-diagnosis attrition was contributed by failure to identify and refer patients. Attrition reduced modestly with time and one factor that might have contributed to this was introduction of CbNAAT in quarter 2 of 2014. General health system strengthening which includes improvement in identification/referral and patient tracking with focus on those with higher risk for not undergoing DST is urgently required.
Keywords: Attrition; Diagnosis and treatment pathway; Diagnosis, delayed; India; Operational research; Tuberculosis, multidrug-resistant/diagnosis; Tuberculosis, multidrug-resistant/prevention and control.
Figures
References
-
- World Health Organization (WHO). Global Tuberculosis Report 2016. Geneva, Switzerland. 2016.
-
- Chadha SS, Sharath BN, Reddy K, Jaju J, Vishnu PH, Rao S, Parmar M, Satyanarayana S, Sachdeva KS, Wilson N, Harries AD. Operational challenges in diagnosing multi-drug resistant TB and initiating treatment in Andhra Pradesh, India. PLoS ONE. 2011;6:e26659. doi: 10.1371/journal.pone.0026659. - DOI - PMC - PubMed
-
- Harries AD, Michongwe J, Nyirenda TE, Kemp JR, Squire SB, Ramsay AR, Godfrey-Faussett P, Salaniponi FM. Using a bus service for transporting sputum specimens to the Central Reference Laboratory: effect on the routine TB culture service in Malawi. Int J Tuberc Lung Dis. 2004;8:204–210. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
