

Definition of common carotid wall thickness affects risk classification in relation to degree of internal carotid artery stenosis: the Plaque At RISK (PARISK) study
- PMID: 28376791
- PMCID: PMC5379498
- DOI: 10.1186/s12947-017-0097-4
Definition of common carotid wall thickness affects risk classification in relation to degree of internal carotid artery stenosis: the Plaque At RISK (PARISK) study
Abstract
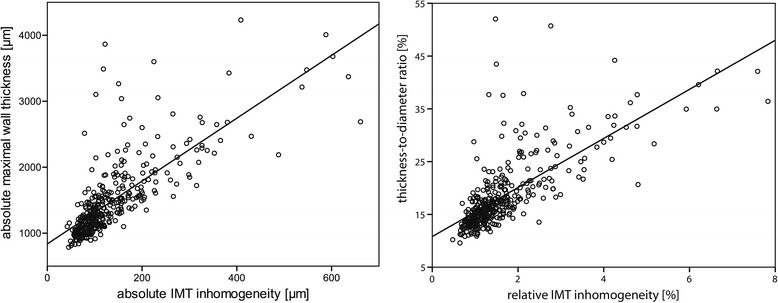
Background: Mean or maximal intima-media thickness (IMT) is commonly used as surrogate endpoint in intervention studies. However, the effect of normalization by surrounding or median IMT or by diameter is unknown. In addition, it is unclear whether IMT inhomogeneity is a useful predictor beyond common wall parameters like maximal wall thickness, either absolute or normalized to IMT or lumen size. We investigated the interrelationship of common carotid artery (CCA) thickness parameters and their association with the ipsilateral internal carotid artery (ICA) stenosis degree.
Methods: CCA thickness parameters were extracted by edge detection applied to ultrasound B-mode recordings of 240 patients. Degree of ICA stenosis was determined from CT angiography.
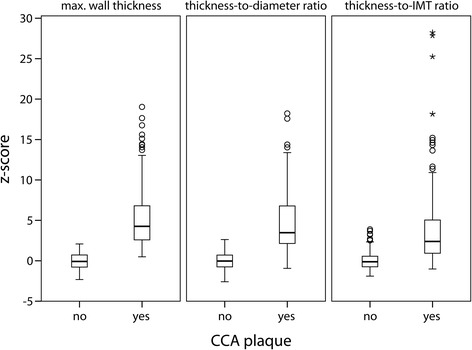
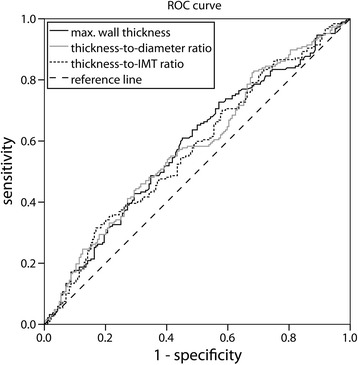
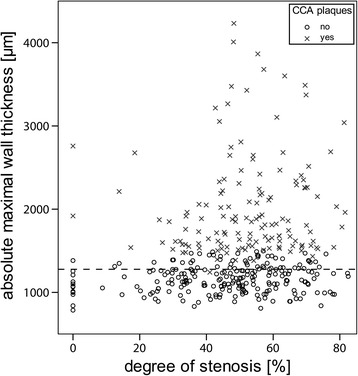
Results: Normalization of maximal CCA wall thickness to median IMT leads to large variations. Higher CCA thickness parameter values are associated with a higher degree of ipsilateral ICA stenosis (p < 0.001), though IMT inhomogeneity does not provide extra information. When the ratio of wall thickness and diameter instead of absolute maximal wall thickness is used as risk marker for having moderate ipsilateral ICA stenosis (>50%), 55 arteries (15%) are reclassified to another risk category.
Conclusions: It is more reasonable to normalize maximal wall thickness to end-diastolic diameter rather than to IMT, affecting risk classification and suggesting modification of the Mannheim criteria.
Trial registration: Clinical trials.gov NCT01208025 .
Keywords: Atherosclerosis; Carotid IMT; Carotid artery imaging; Stenosis; Ultrasound.
Figures
References
-
- Steinbuch J, van Dijk AC, Schreuder FH, Truijman MT, de Rotte AA, Nederkoorn PJ, van der Lugt A, Hermeling E, Hoeks AP, Mess WH. High Spatial Inhomogeneity in the Intima-Media Thickness of the Common Carotid Artery is Associated with a Larger Degree of Stenosis in the Internal Carotid Artery: The PARISK Study. Ultraschall in der Medizin 2016. doi:10.1055/s-0042-112220. - PubMed
-
- Saba L, Meiburger KM, Molinari F, Ledda G, Anzidei M, Acharya UR, Zeng G, Shafique S, Nicolaides A, Suri JS. Carotid IMT variability (IMTV) and its validation in symptomatic versus asymptomatic Italian population: can this be a useful index for studying symptomaticity? Echocardiography. 2012;29(9):1111–1119. doi: 10.1111/j.1540-8175.2012.01763.x. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
