

Impact of diabetes on outcome in critical limb ischemia with tissue loss: a large-scaled routine data analysis
- PMID: 28376797
- PMCID: PMC5379505
- DOI: 10.1186/s12933-017-0524-8
Impact of diabetes on outcome in critical limb ischemia with tissue loss: a large-scaled routine data analysis
Abstract
Background: Patients with diabetes concomitant to critical limb ischemia (CLI) represent a sub-group at particular risk. Objective of this analysis is to evaluate the actual impact of diabetes on treatment, outcome, and costs in a real-world scenario in Germany.
Methods: We obtained routine-data on 15,332 patients with CLI with tissue loss from the largest German health insurance, BARMER GEK from 2009 to 2011, including a follow-up until 2013. Patient data were analyzed regarding co-diagnosis with diabetes with respect to risk profiles, treatment strategy, in-hospital and long-term outcome including costs.
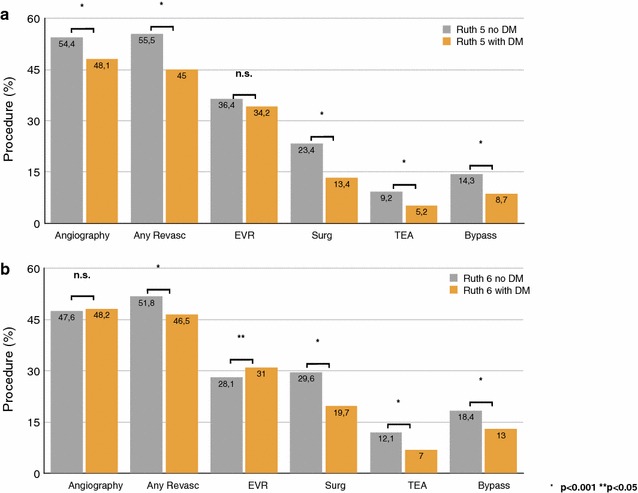
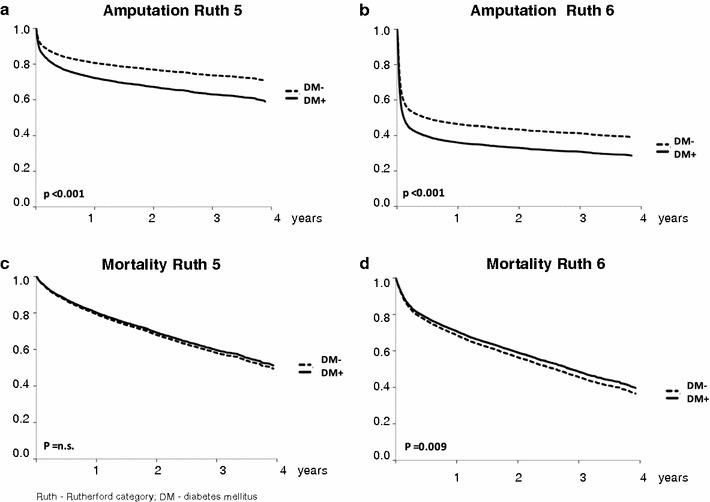
Results: Diabetic patients received less overall revascularizations in Rutherford grades 5 and 6 (Rutherford grade 5: 45.0 vs. 55.5%; Rutherford grade 6: 46.5 vs. 51.8; p < 0.001) and less vascular surgery (Rutherford grade 5: 13.4 vs. 23.4; Rutherford grade 6: 19.7 vs. 29.6; p < 0.001), however more often endovascular revascularization in Rutherford grade 6 (31.0 vs. 28.1; p = 0.004) compared to non-diabetic patients. Diabetes was associated with a higher observed ratio of infections (35.3 vs. 23.5% Rutherford grade 5; 44.3 vs. 27.4% Rutherford grade 6; p < 0.001) and in-hospital amputations (13.0 vs. 7.3% Rutherford grade 5; 47.5 vs. 36.7% Ruth6; p < 0.001). Diabetes further increased the risk for amputation during follow-up [Rutherford grade 5: HR 1.51 (1.38-1.67); Rutherford grade 6: HR 1.33 (1.25-1.41); p < 0.001], but not for death.
Conclusions: Diabetes increases markedly the risk of amputation attended by higher costs in CLI patients with tissue loss (OR 1.67 at Rutherford 5, OR 1.53 at Rutherford 6; p < 0.001), but is associated with lower revascularizations. However, in Rutherford grades 5 and 6, concomitant diabetes does not further worsen the overall poor survival.
Keywords: Critical limb ischemia; Diabetes; Epidemiology; Outcome; Routine-data analysis.
Figures
References
-
- Lawall H, Huppert P, Rümenapf G und weitere Mitglieder der Leitliniengruppe. S3-Leitlinie zur Diagnostik, Therapie und Nachsorge der peripheren arteriellen Verschlusskrankheit. AWMF-Registernummer 065-003. 2015. http://www.dga-gefaessmedizin.de/uploads/media/S3_PAVK_15-11-30.pdf. Accessed 7 Dec 2016.
-
- European Stroke Organisation. Tendera M, Aboyans V, Bartelink ML, Baumgartner I, Clément D, Collet JP, Cremonesi A, De Carlo M, Erbel R, Fowkes FG, Heras M, Kownator S, Minar E, Ostergren J, Poldermans D, Riambau V, Roffi M, Röther J, Sievert H, van Sambeek M, Zeller T, ESC Committee for Practice Guidelines ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the task force on the diagnosis and treatment of peripheral artery diseases of the European Society of Cardiology (ESC) Eur Heart J. 2011;32(22):2851–2906. doi: 10.1093/eurheartj/ehr211. - DOI - PubMed
-
- Malyar N, Fürstenberg T, Wellmann J, Meyborg M, Lüders F, Gebauer K, Bunzemeier H, Roeder N, Reinecke H. Recent trends in morbidity and in-hospital outcomes of in-patients with peripheral arterial disease: a nationwide population-based analysis. Eur Heart J. 2013;34(34):2706–2714. doi: 10.1093/eurheartj/eht288. - DOI - PubMed
-
- Reinecke H, Unrath M, Freisinger E, Bunzemeier H, Meyborg M, Lüders F, Gebauer K, Roeder N, Berger K, Malyar NM. Peripheral arterial disease and critical limb ischaemia: still poor outcomes and lack of guideline adherence. Eur Heart J. 2015;36(15):932–938. doi: 10.1093/eurheartj/ehv006. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
