

Quantifying the Release of Biomarkers of Myocardial Necrosis from Cardiac Myocytes and Intact Myocardium
- PMID: 28377413
- PMCID: PMC6114147
- DOI: 10.1373/clinchem.2016.264648
Quantifying the Release of Biomarkers of Myocardial Necrosis from Cardiac Myocytes and Intact Myocardium
Abstract
Background: Myocardial infarction is diagnosed when biomarkers of cardiac necrosis exceed the 99th centile, although guidelines advocate even lower concentrations for early rule-out. We examined how many myocytes and how much myocardium these concentrations represent. We also examined if dietary troponin can confound the rule-out algorithm.
Methods: Individual rat cardiac myocytes, rat myocardium, ovine myocardium, or human myocardium were spiked into 400-μL aliquots of human serum. Blood was drawn from a volunteer after ingestion of ovine myocardium. High-sensitivity assays were used to measure cardiac troponin T (cTnT; Roche, Elecsys), cTnI (Abbott, Architect), and cardiac myosin-binding protein C (cMyC; EMD Millipore, Erenna®).
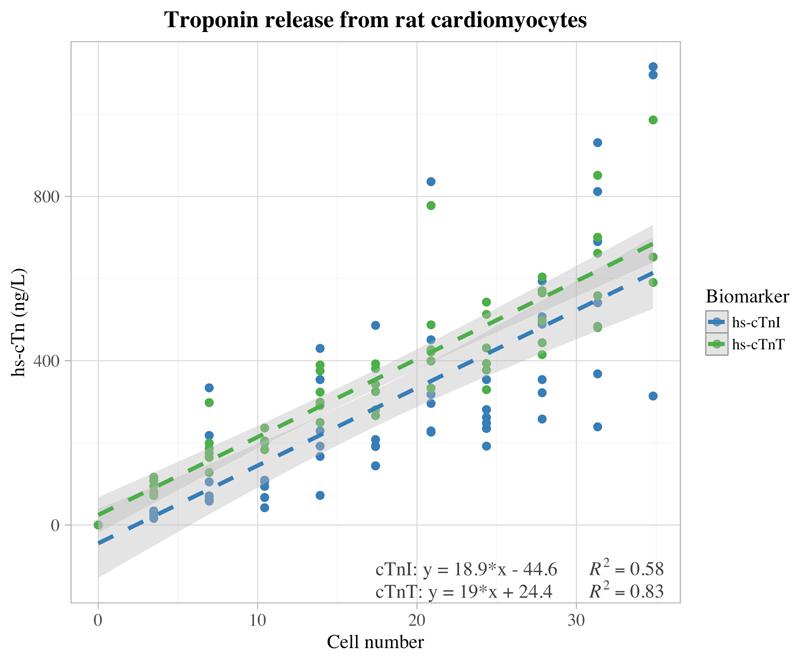
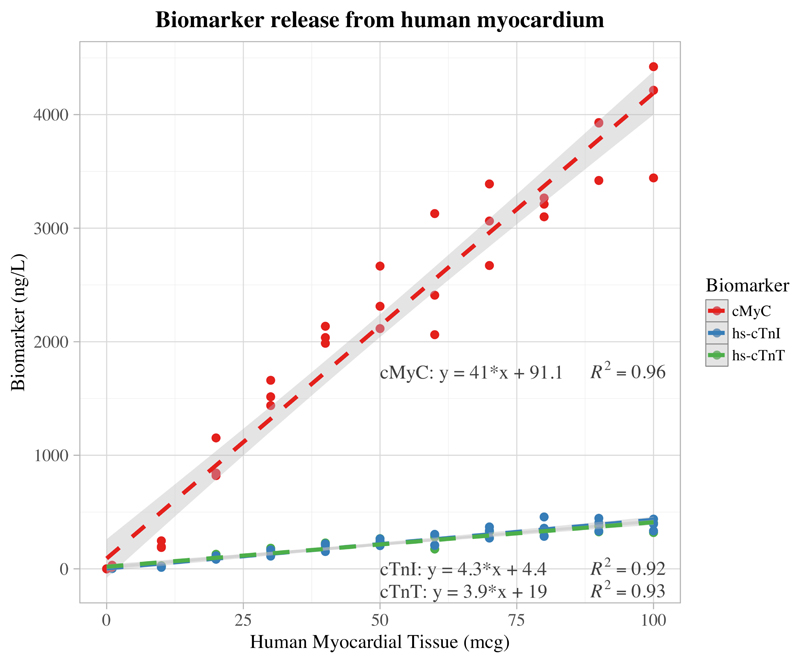
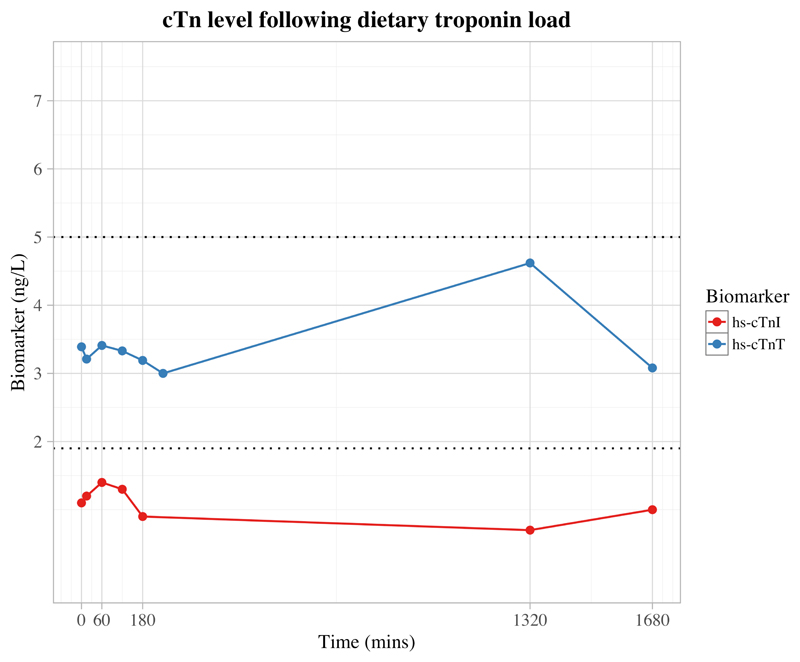
Results: The cMyC assay could only detect the human protein. For each rat cardiac myocyte added to 400 μL of human serum, cTnT and cTnI increased by 19.0 ng/L (95% CI, 16.8-21.2) and 18.9 ng/L (95% CI, 14.7-23.1), respectively. Under identical conditions cTnT, cTnI, and cMyC increased by 3.9 ng/L (95% CI, 3.6-4.3), 4.3 ng/L (95% CI, 3.8-4.7), and 41.0 ng/L (95% CI, 38.0-44.0) per μg of human myocardium. There was no detectable change in cTnI or cTnT concentration after ingestion of sufficient ovine myocardium to increase cTnT and cTnI to approximately 1 × 108 times their lower limits of quantification.
Conclusions: Based on pragmatic assumptions regarding cTn and cMyC release efficiency, circulating species, and volume of distribution, 99th centile concentrations may be exceeded by necrosis of 40 mg of myocardium. This volume is much too small to detect by noninvasive imaging.
© 2017 American Association for Clinical Chemistry.
Conflict of interest statement
Millipore Sigma (Hayward, California) was contracted to undertake the analyses of cMyC on a fee-for-service basis and hold no commercial interest. Marber is named as an inventor on a patent held by King’s College London for the detection of cMyC as a biomarker of myocardial injury.
Figures
References
-
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60:1581–98. - PubMed
-
- Roffi M, Patrono C, Collet J-P, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) Eur Heart J. 2016;37:267–315. - PubMed
-
- Reichlin T, Schindler C, Drexler B, Twerenbold R, Reiter M, Zellweger C, et al. One-Hour Rule-out and Rule-in of Acute Myocardial Infarction Using High-Sensitivity Cardiac Troponin T. Arch Intern Med. 2012;172:1211–8. - PubMed
-
- Rubini Giménez M, Twerenbold R, Jaeger C, Schindler C, Puelacher C, Wildi K, et al. One-hour rule-in and rule-out of acute myocardial infarction using high-sensitivity cardiac troponin I. Am J Med. 2015;128:861–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
