

Development and clinical utility of a novel diagnostic nystagmus gene panel using targeted next-generation sequencing
- PMID: 28378818
- PMCID: PMC5477371
- DOI: 10.1038/ejhg.2017.44
Development and clinical utility of a novel diagnostic nystagmus gene panel using targeted next-generation sequencing
Abstract
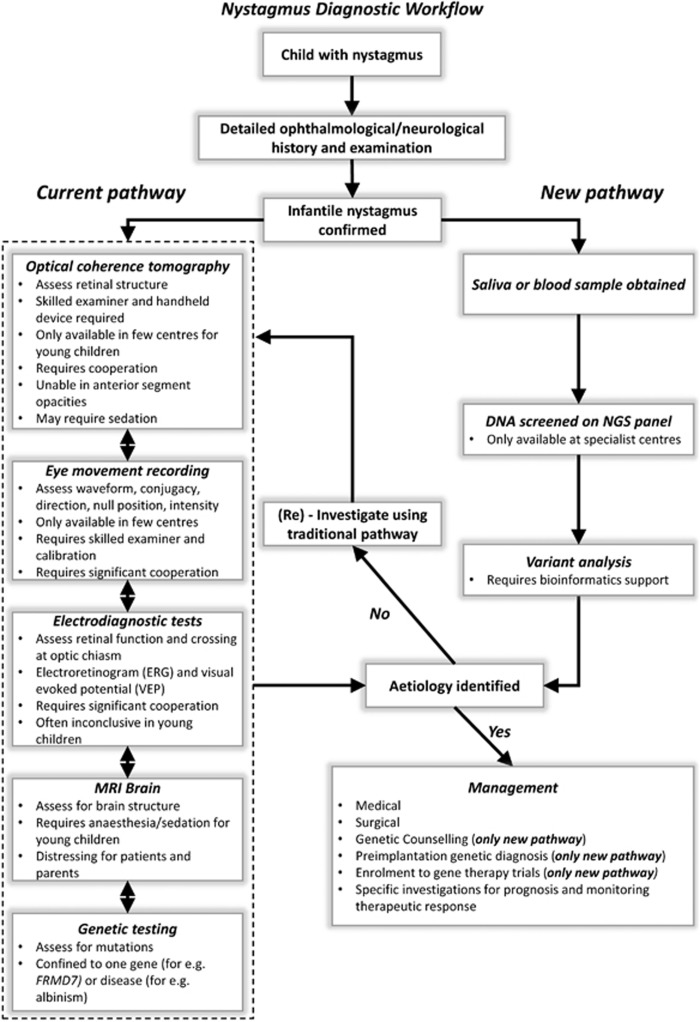
Infantile nystagmus (IN) is a genetically heterogeneous disorder arising from variants of genes expressed within the developing retina and brain. IN presents a diagnostic challenge and patients often undergo numerous investigations. We aimed to develop and assess the utility of a next-generation sequencing (NGS) panel to enhance the diagnosis of IN. We identified 336 genes associated with IN from the literature and OMIM. NimbleGen Human custom array was used to enrich the target genes and sequencing was performed using HiSeq2000. Using reference genome material (NA12878), we show the sensitivity (98.5%) and specificity (99.9%) of the panel. Fifteen patients with familial IN were sequenced using the panel. Two authors were masked to the clinical diagnosis. We identified variants in 12/15 patients in the following genes: FRMD7 (n=3), CACNA1F (n=2), TYR (n=5), CRYBA1 (n=1) and TYRP1 (n=1). In 9/12 patients, the clinical diagnosis was consistent with the genetic diagnosis. In 3/12 patients, the results from the genetic diagnoses (TYR, CRYBA1 and TYRP1 variants) enabled revision of clinical diagnoses. In 3/15 patients, we were unable to determine a genetic diagnosis. In one patient, copy number variation analysis revealed a FRMD7 deletion. This is the first study establishing the clinical utility of a diagnostic NGS panel for IN. We show that the panel has high sensitivity and specificity. The genetic information from the panel will lead to personalised diagnosis and management of IN and enable accurate genetic counselling. This will allow development of a new clinical care pathway for IN.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Sarvananthan N, Surendran M, Roberts EO et al: The prevalence of nystagmus: the Leicestershire nystagmus survey. Invest Ophthalmol Vis Sci 2009; 50: 5201–5206. - PubMed
-
- McLean RJ, Windridge KC, Gottlob I: Living with nystagmus: a qualitative study. Br J Ophthalmol 2012; 96: 981–986. - PubMed
-
- Gottlob I: Nystagmus. Curr Opin Ophthalmol 2000; 11: 330–335. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
