

Characteristics, outcomes, prognostic factors and treatment of patients with T-cell prolymphocytic leukemia (T-PLL)
- PMID: 28379307
- PMCID: PMC5834082
- DOI: 10.1093/annonc/mdx163
Characteristics, outcomes, prognostic factors and treatment of patients with T-cell prolymphocytic leukemia (T-PLL)
Abstract
Background: T-cell prolymphocytic leukemia (T-PLL) is a rare and aggressive disease. In this study, we report our experience from 119 patients with T-PLL.
Patients and methods: We reviewed the clinico-pathologic records of 119 consecutive patients with T-PLL, who presented to our institution between 1990 and 2016.
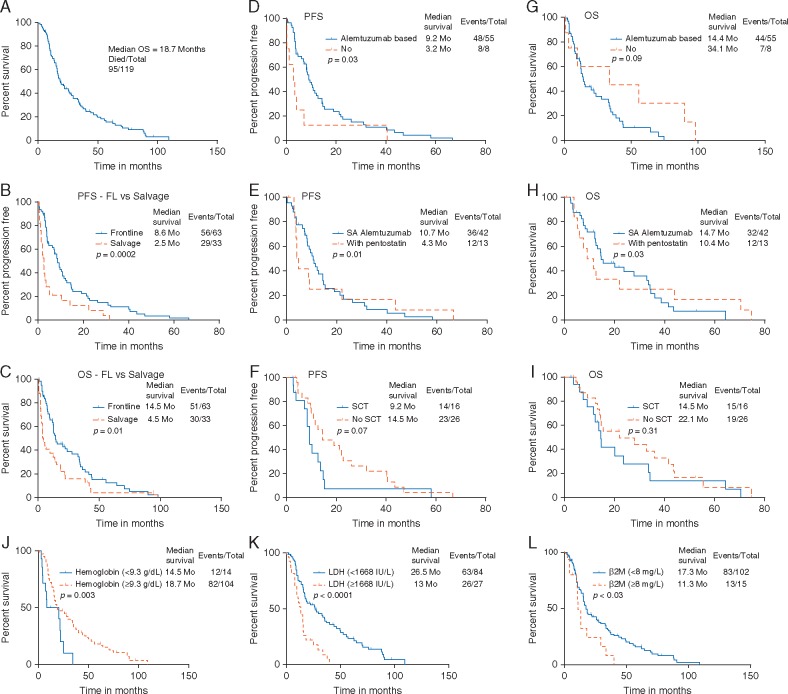
Results: One hundred and nineteen patients with T-PLL were analysed. Complex karyotype and aberrations in chromosome 14 were seen in 65% and 52% patients, respectively. Seventy-five patients (63%) were previously untreated and 43 (37%) were initially treated outside our institution. Sixty-three previously untreated patients (84%) received frontline therapies. Overall, 95 patients (80%) have died. Median overall survival (OS) from diagnosis was 19 months [95% confidence interval (CI) 16-26 months]. Using recursive partitioning (RP), we found that patients with hemoglobin < 9.3 g/dl, lactate dehydrogenase (LDH) ≥ 1668 IU/l, white blood cell ≥ 208 K/l and β2M ≥ 8 mg/l had significantly inferior OS and patients with hemoglobin < 9.3 g/dl had inferior progression-free survival (PFS). In multivariate analysis, we identified that presence of pleural effusion [hazard ratio (HR) 2.08 (95% CI 1.11-3.9); P = 0.02], high LDH (≥ 1668 IU/l) [HR 2.5 (95% CI 1.20-4.24); P < 0.001)], and low hemoglobin (< 9.3 g/dl) [HR 0.33 (95% CI 0.14-0.75); P = 0.008] were associated with shorter OS. Fifty-five previously untreated patients received treatment with an alemtuzumab-based regimen (42 monotherapy and 13 combination with pentostatin). Overall response rate, complete remission rate (CR) for single-agent alemtuzumab and alemtuzumab combined with pentostatin were 83%, 66% and 82%, 73% respectively. In patients who achieved initial CR, stem cell transplantation was not associated with longer PFS and OS.
Conclusion: Outcomes in T-PLL remain poor. Multicenter collaborative effort is required to conduct prospective studies.
Keywords: T-PLL; prolymphocytes; prolymphocytic leukemia.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Chen X, Cherian S.. Immunophenotypic characterization of T-cell prolymphocytic leukemia. Am J Clin Pathol 2013; 140: 727–735. - PubMed
-
- Dearden C. Management of prolymphocytic leukemia. Hematol Am Soc Hematol Educ Program 2015; 2015: 361–367. - PubMed
-
- Urbankova H, Holzerova M, Balcarkova J. et al. Array comparative genomic hybridization in the detection of chromosomal abnormalities in T-cell prolymphocytic leukemia. Cancer Genet Cytogenet 2010; 202: 58–62. - PubMed
-
- Auguin D, Barthe P, Royer C. et al. Structural basis for the co-activation of protein kinase B by T-cell leukemia-1 (TCL1) family proto-oncoproteins. J Biol Chem 2004; 279: 35890–35902. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
