

Editorial
doi: 10.1093/eurheartj/ehx122.
Subclinical atrial fibrillation in need of more assertive evidence
Affiliations
- PMID: 28379323
- PMCID: PMC5837597
- DOI: 10.1093/eurheartj/ehx122
Item in Clipboard
Editorial
Subclinical atrial fibrillation in need of more assertive evidence
Eur Heart J.
.
No abstract available
Figures
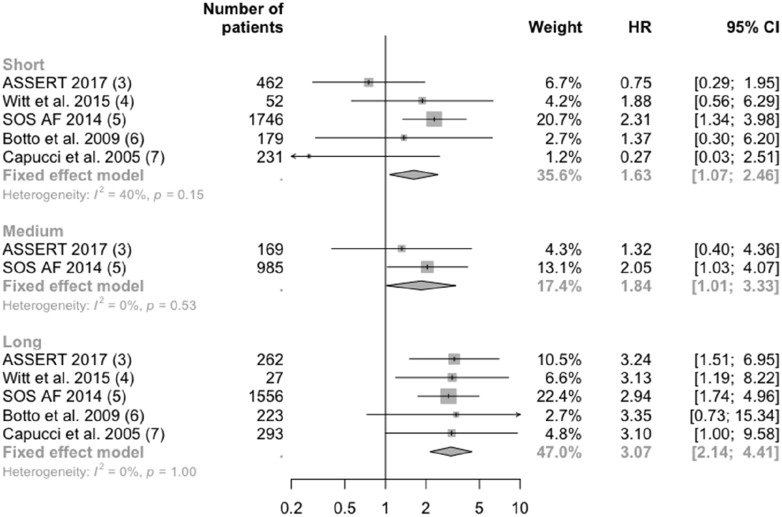
Association of risk of stroke and embolism by categories of duration of subclinical atrial fibrillation (AF). Inclusion criteria for patients were: Witt et al., implantable cardioverter defibrillator (ICD) and no clinical AF; SOS AF, implantable devices and no clinical AF; Botto et al., pacemaker and history of AF; Capucci et al., patients with bradycardic pacing; ASSERT, pacemaker, history of hypertension, older than 65 years, and no history of AF. Witt et al., Botto et al., and Capucci et al. chose stroke, transient ischaemic attack (TIA), and peripheral arterial embolism as their outcome. SOS AF chose ischaemic stroke and TIA. ASSERT chose stroke and systemic embolism. Short duration of subclinical AF is defined as 6 min to 24 h in Witt et al., 5 min to 24 h in Botto et al. and Cappuci et al., 5 min to 6 h in SOS AF, and 6 min to 6 h in ASSERT. Medium duration of subclinical AF is defined as 6–23 h in SOS AF and 6–24 h in ASSERT. Long duration of subclinical AF is defined as > 23 h in SOS AF and >24 h in all other studies. CI, confidence interval; HR, hazard ratio.
Comment on
-
Duration of device-detected subclinical atrial fibrillation and occurrence of stroke in ASSERT.Eur Heart J. 2017 May 1;38(17):1339-1344. doi: 10.1093/eurheartj/ehx042. Eur Heart J. 2017. PMID: 28329139
References
-
- Chen-Scarabelli C, Scarabelli TM, Ellenbogen KA, Halperin JL.. Device-detected atrial fibrillation. J Am Coll Cardiol 2015;65:281–294. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K.. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothoracic Surg 2016;50:e1–e88. - PubMed
-
- Van Gelder IC, Healey JS, Crijns HJGM, Wang J, Hohnloser SH, Gold MR, Capucci A, Lau C-P, Morillo CA, Hobbelt AH, Rienstra M, Connolly SJ. Duration of device-detected subclinical atrial fibrillation and occurrence of stroke in ASSERT. Eur Heart J 2017;38:1339–1344. - PubMed
-
- Witt CT, Kronborg MB, Nohr EA, Mortensen PT, Gerdes C, Nielsen JC.. Early detection of atrial high rate episodes predicts atrial fibrillation and thromboembolic events in patients with cardiac resynchronization therapy. Hear Rhythm 2015;12:2368–2375. - PubMed
-
- Boriani G, Glotzer TV, Santini M, West TM, De Melis M, Sepsi M, Gasparini M, Lewalter T, Camm JA, Singer DE.. Device-detected atrial fibrillation and risk for stroke: an analysis of > 10 000 patients from the SOS AF project (Stroke preventiOn Strategies based on Atrial Fibrillation information from implanted devices). Eur Heart J 2014;35:508–516. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
