

Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma
- PMID: 28379796
- PMCID: PMC6201242
- DOI: 10.1056/NEJMoa1611750
Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma
Abstract
Background: High-dose chemotherapy plus autologous stem-cell transplantation has been the standard treatment for newly diagnosed multiple myeloma in adults up to 65 years of age. However, promising data on the use of combination therapy with lenalidomide, bortezomib, and dexamethasone (RVD) in this population have raised questions about the role and timing of transplantation.
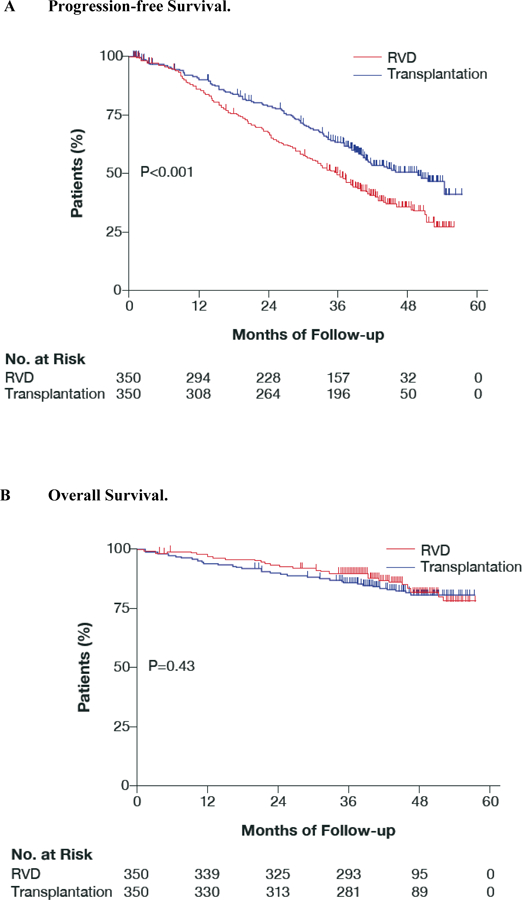
Methods: We randomly assigned 700 patients with multiple myeloma to receive induction therapy with three cycles of RVD and then consolidation therapy with either five additional cycles of RVD (350 patients) or high-dose melphalan plus stem-cell transplantation followed by two additional cycles of RVD (350 patients). Patients in both groups received maintenance therapy with lenalidomide for 1 year. The primary end point was progression-free survival.
Results: Median progression-free survival was significantly longer in the group that underwent transplantation than in the group that received RVD alone (50 months vs. 36 months; adjusted hazard ratio for disease progression or death, 0.65; P<0.001). This benefit was observed across all patient subgroups, including those stratified according to International Staging System stage and cytogenetic risk. The percentage of patients with a complete response was higher in the transplantation group than in the RVD-alone group (59% vs. 48%, P=0.03), as was the percentage of patients in whom minimal residual disease was not detected (79% vs. 65%, P<0.001). Overall survival at 4 years did not differ significantly between the transplantation group and the RVD-alone group (81% and 82%, respectively). The rate of grade 3 or 4 neutropenia was significantly higher in the transplantation group than in the RVD-alone group (92% vs. 47%), as were the rates of grade 3 or 4 gastrointestinal disorders (28% vs. 7%) and infections (20% vs. 9%). No significant between-group differences were observed in the rates of treatment-related deaths, second primary cancers, thromboembolic events, and peripheral neuropathy.
Conclusions: Among adults with multiple myeloma, RVD therapy plus transplantation was associated with significantly longer progression-free survival than RVD therapy alone, but overall survival did not differ significantly between the two approaches. (Supported by Celgene and others; IFM 2009 Study ClinicalTrials.gov number, NCT01191060 .).
Figures

Comment in
-
Haematological cancer: Where are we now with the treatment of multiple myeloma?Nat Rev Clin Oncol. 2017 Aug;14(8):461-462. doi: 10.1038/nrclinonc.2017.82. Epub 2017 Jun 13. Nat Rev Clin Oncol. 2017. PMID: 28607521 No abstract available.
-
Drug Combinations with Transplantation for Myeloma.N Engl J Med. 2017 Jul 6;377(1):91-2. doi: 10.1056/NEJMc1705671. N Engl J Med. 2017. PMID: 28679086 No abstract available.
-
Drug Combinations with Transplantation for Myeloma.N Engl J Med. 2017 Jul 6;377(1):92. doi: 10.1056/NEJMc1705671. N Engl J Med. 2017. PMID: 28679087 No abstract available.
-
Drug Combinations with Transplantation for Myeloma.N Engl J Med. 2017 Jul 6;377(1):92-3. doi: 10.1056/NEJMc1705671. N Engl J Med. 2017. PMID: 28691787 No abstract available.
References
-
- Attal M, Harousseau JL, Stoppa AM, et al. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. N Engl J Med 1996;335:91–97. - PubMed
-
- Child JA, Morgan GJ, Davies FE, et al. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl Med 2003;348:1875–83. - PubMed
-
- Facon T, Mary JY, Hulin C, et al. Melphalan and prednisone plus thalidomide versus melphalan and prednisone alone or reduced-intensity autologous stem cell transplantation in elderly patients with multiple myeloma (IFM 99–06): a randomised trial. Lancet 2007;370:1209–18. - PubMed
-
- Hulin C, Facon T, Rodon P, et al. Efficacy of melphalan and prednisone plus thalidomide in patients older than 75 years with newly diagnosed multiple myeloma: IFM 01/01 trial. J Clin Oncol 2009;27:3664–70. - PubMed
-
- Palumbo A, Bringhen S, Caravita T, et al. Italian Multiple Myeloma Network, GIMEMA. Oral melphalan and prednisone chemotherapy plus thalidomide compared with melphalan and prednisone alone in elderly patients with multiple myeloma: randomised controlled trial. Lancet 2006; 367:825–31. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical