

Response of the human myocardium to ischemic injury and preconditioning: The role of cardiac and comorbid conditions, medical treatment, and basal redox status
- PMID: 28380047
- PMCID: PMC5381881
- DOI: 10.1371/journal.pone.0174588
Response of the human myocardium to ischemic injury and preconditioning: The role of cardiac and comorbid conditions, medical treatment, and basal redox status
Abstract
Background: The diseased human myocardium is highly susceptible to ischemia/reoxygenation (I/R)-induced injury but its response to protective interventions such as ischemic preconditioning (IPreC) is unclear. Cardiac and other pre-existing clinical conditions as well as previous or ongoing medical treatment may influence the myocardial response to I/R injury and protection. This study investigated the effect of both on myocardial susceptibility to I/R-induced injury and the protective effects of IPreC.
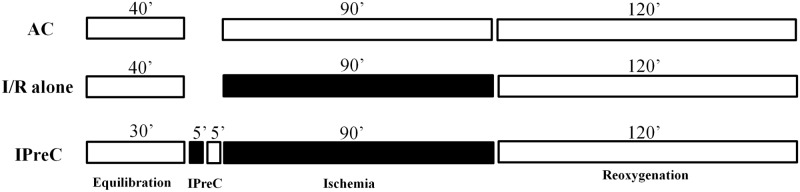
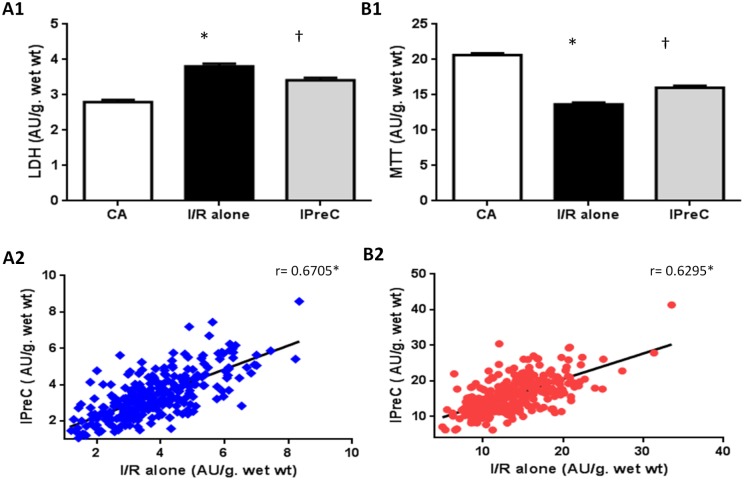
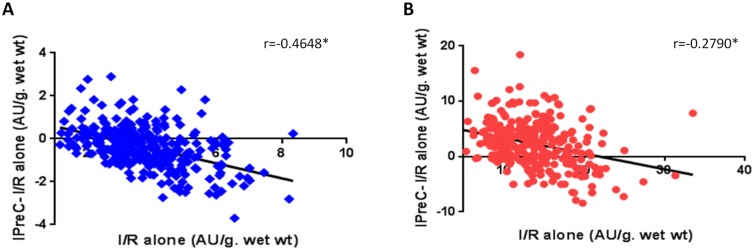
Methods and results: Atrial myocardium from cardiac surgery patients (n = 300) was assigned to one of three groups: aerobic control, I/R alone, and IPreC. Lactate dehydrogenase leakage, as a marker of cell injury, and cell viability were measured. The basal redox status was determined in samples from 90 patients. The response to I/R varied widely. Myocardium from patients with aortic valve disease was the most susceptible to injury whereas myocardium from dyslipidemia patients was the least susceptible. Tissue from females was better protected than tissue from males. Myocardium from patients with mitral valve disease was the least responsive to IPreC. The basal redox status was altered in the myocardium from patients with mitral and aortic valve disease.
Conclusions: The response of the myocardium to I/R and IPreC is highly variable and influenced by the underlying cardiac pathology, dyslipidemia, sex, and the basal redox status. These results should be taken into account in the design of future clinical studies on the prevention of I/R injury and protection.
Conflict of interest statement
Figures
Similar articles
-
The aging human myocardium: tolerance to ischemia and responsiveness to ischemic preconditioning.J Thorac Cardiovasc Surg. 2003 Jul;126(1):143-7. doi: 10.1016/s0022-5223(02)73601-5. J Thorac Cardiovasc Surg. 2003. PMID: 12878949 Clinical Trial.
-
Protective Effect of Ischemic Preconditioning on Myocardium Against Remote Tissue Injury Following Transient Focal Cerebral Ischemia in Diabetic Rats.Arq Bras Cardiol. 2017 Dec;109(6):516-526. doi: 10.5935/abc.20170164. Epub 2017 Nov 13. Arq Bras Cardiol. 2017. PMID: 29160389 Free PMC article.
-
Preconditioning the hyperlipidemic myocardium: fact or fantasy?Cell Signal. 2012 Mar;24(3):589-95. doi: 10.1016/j.cellsig.2011.11.003. Epub 2011 Nov 9. Cell Signal. 2012. PMID: 22101013 Review.
-
Ferilnic nirate produces delayed preconditioning against myocardial ischemia and reperfusion injury in rats.Arch Pharm Res. 2010 Jun;33(6):881-7. doi: 10.1007/s12272-010-0611-9. Epub 2010 Jul 6. Arch Pharm Res. 2010. PMID: 20607493
-
Pharmacological preconditioning with hyperbaric oxygen: can this therapy attenuate myocardial ischemic reperfusion injury and induce myocardial protection via nitric oxide?J Surg Res. 2008 Sep;149(1):155-64. doi: 10.1016/j.jss.2007.09.003. Epub 2007 Oct 11. J Surg Res. 2008. PMID: 17996900 Review.
Cited by
-
Role of Erythropoiesis-Stimulating Agents in Cardiovascular Protection in CKD Patients: Reappraisal of Their Impact and Mechanisms.Cardiovasc Drugs Ther. 2023 Dec;37(6):1175-1192. doi: 10.1007/s10557-022-07321-3. Epub 2022 Feb 12. Cardiovasc Drugs Ther. 2023. PMID: 35150385 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
