

Metformin inhibits proliferation and growth hormone secretion of GH3 pituitary adenoma cells
- PMID: 28380462
- PMCID: PMC5514928
- DOI: 10.18632/oncotarget.16556
Metformin inhibits proliferation and growth hormone secretion of GH3 pituitary adenoma cells
Abstract
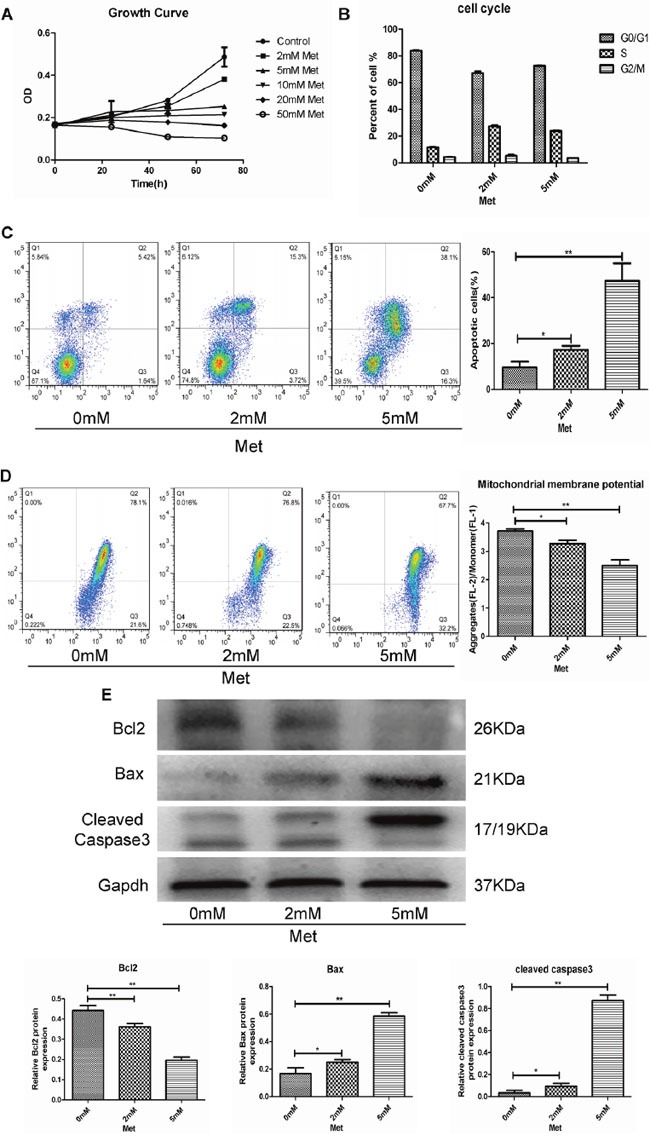
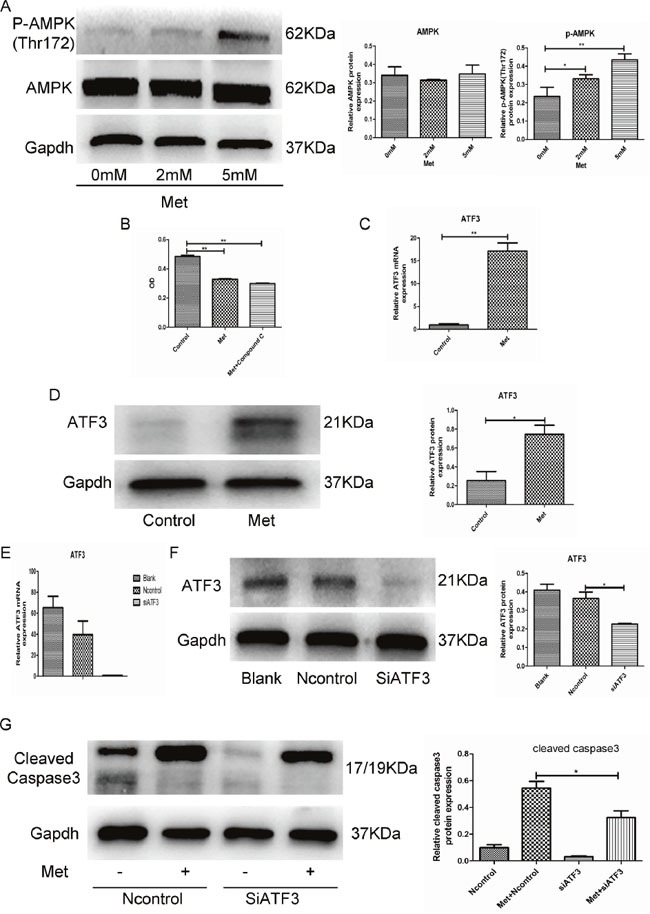
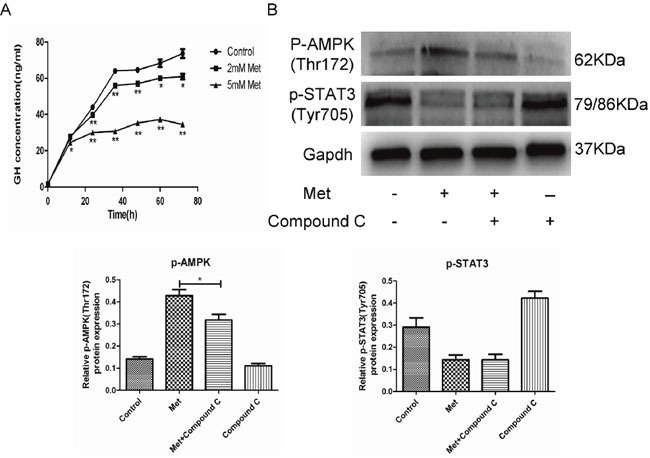
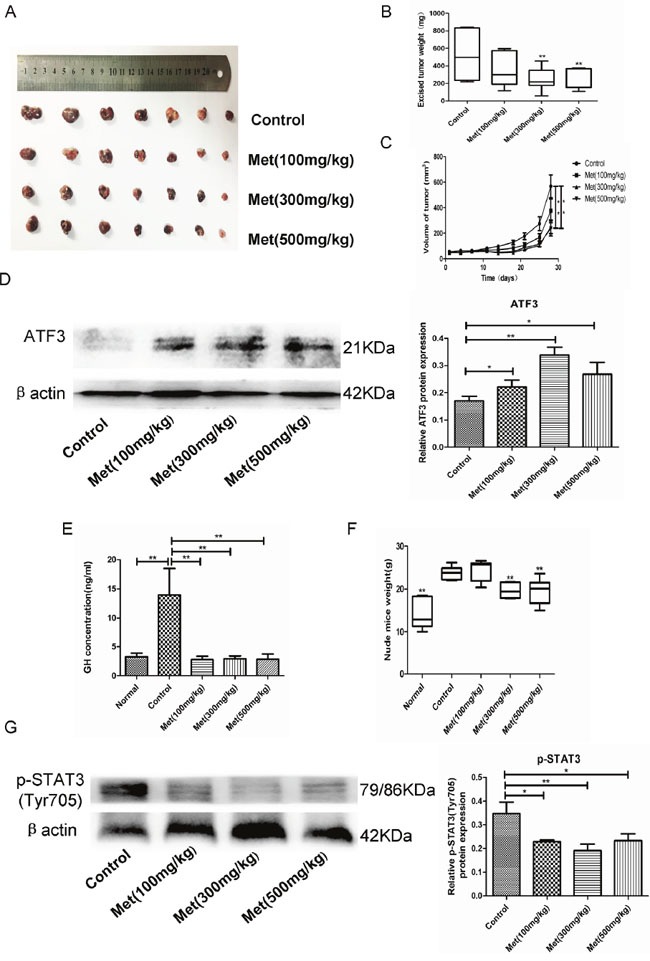
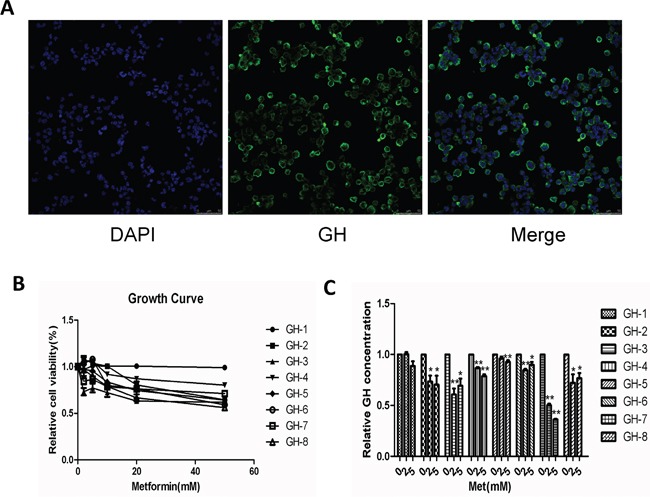
Metformin is an anti-hyperglycemic agent used to treat diabetes, and recent evidence suggests it has antitumor efficacy. Because growth hormone-secreting pituitary adenoma (GH-PA) patients have a high incidence of diabetes frequently treated with metformin, we assessed the antitumor effect of metformin on GH-PA. We found that metformin effectively inhibited proliferation and induced apoptosis in the GH-PA cell line GH3. We detected a decrease in mitochondrial membrane potential (MMP), an increase in expression of pro-apoptotic proteins, and a decrease in expression of an anti-apoptotic protein in metformin-treated GH3 cells, which suggests involvement of the mitochondrial-mediated apoptosis pathway. Inhibition of AMPK, which is activated by metformin, failed to reverse the antiproliferative effect. ATF3 was upregulated by metformin, and its knockdown significantly reduced metformin-induced apoptosis. In addition, GH secretion was inhibited by metformin through suppression of STAT3 activity independently of AMPK. Metformin also significantly suppressed cellular proliferation and GH secretion in primary human GH-PA cells. Metformin also significantly inhibited GH3 cell proliferation and GH secretion in vivo. ATF3 upregulation and p-STAT3 downregulation were confirmed in xenografts. These findings suggest metformin is a potentially promising therapeutic agent for the treatment of GH-PA, particularly in patients with diabetes.
Keywords: ATF3; STAT3; growth hormone-secreting pituitary adenoma; metformin; proliferation.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
The CXCR4 antagonist AMD3100 suppresses hypoxia-mediated growth hormone production in GH3 rat pituitary adenoma cells.J Neurooncol. 2010 Oct;100(1):51-64. doi: 10.1007/s11060-010-0152-6. Epub 2010 Mar 23. J Neurooncol. 2010. PMID: 20309720
-
Inhibition of PI3K/AKT/mTOR pathway enhances temozolomide-induced cytotoxicity in pituitary adenoma cell lines in vitro and xenografted pituitary adenoma in female nude mice.Endocrinology. 2013 Mar;154(3):1247-59. doi: 10.1210/en.2012-1908. Epub 2013 Feb 5. Endocrinology. 2013. PMID: 23384836
-
Role of KCNAB2 expression in modulating hormone secretion in somatotroph pituitary adenoma.J Neurosurg. 2020 Feb 28;134(3):787-793. doi: 10.3171/2019.12.JNS192435. Print 2021 Mar 1. J Neurosurg. 2020. PMID: 32109873
-
STAT3 upregulation in pituitary somatotroph adenomas induces growth hormone hypersecretion.J Clin Invest. 2015 Apr;125(4):1692-702. doi: 10.1172/JCI78173. Epub 2015 Mar 16. J Clin Invest. 2015. PMID: 25774503 Free PMC article.
-
Emerging role of signal transducer and activator of transcription 3 (STAT3) in pituitary adenomas.Endocr J. 2021 Oct 28;68(10):1143-1153. doi: 10.1507/endocrj.EJ21-0106. Epub 2021 Jul 10. Endocr J. 2021. PMID: 34248112 Review.
Cited by
-
The role of an anti-diabetic drug metformin in the treatment of endocrine tumors.J Mol Endocrinol. 2019 Aug;63(2):R17-R35. doi: 10.1530/JME-19-0083. J Mol Endocrinol. 2019. PMID: 31307011 Free PMC article. Review.
-
How treatments with endocrine and metabolic drugs influence pituitary cell function.Endocr Connect. 2020 Feb;9(2):R14-R27. doi: 10.1530/EC-19-0482. Endocr Connect. 2020. PMID: 31905162 Free PMC article. Review.
-
MicroRNA-186 targets SKP2 to induce p27Kip1-mediated pituitary tumor cell cycle deregulation and modulate cell proliferation.Korean J Physiol Pharmacol. 2019 May;23(3):171-179. doi: 10.4196/kjpp.2019.23.3.171. Epub 2019 Apr 24. Korean J Physiol Pharmacol. 2019. PMID: 31080348 Free PMC article.
-
Metformin inhibits growth and prolactin secretion of pituitary prolactinoma cells and xenografts.J Cell Mol Med. 2018 Dec;22(12):6368-6379. doi: 10.1111/jcmm.13963. Epub 2018 Oct 18. J Cell Mol Med. 2018. PMID: 30334324 Free PMC article.
-
Drug Repositioning for Refractory Benign Tumors of the Central Nervous System.Int J Mol Sci. 2023 Aug 20;24(16):12997. doi: 10.3390/ijms241612997. Int J Mol Sci. 2023. PMID: 37629179 Free PMC article. Review.
References
-
- Schneider HJ, Sievers C, Saller B, Wittchen HU, Stalla GK. High prevalence of biochemical acromegaly in primary care patients with elevated IGF-1 levels. Clin Endocrinol. 2008;69:432–435. - PubMed
-
- Rosario PW. Frequency of acromegaly in adults with diabetes or glucose intolerance and estimated prevalence in the general population. Pituitary. 2011;14:217–221. - PubMed
-
- Melmed S. Medical progress: acromegaly. N Engl J Med. 2006;355:2558–2573. - PubMed
-
- Damjanovic SS, Neskovic AN, Petakov MS, Popovic V, Vujisic B, Petrovic M, Nikolic-Djurovic M, Simic M, Pekic S, Marinkovic J. High output heart failure in patients with newly diagnosed acromegaly. Am J Med. 2002;112:610–616. - PubMed
-
- Bihan H, Espinosa C, Valdes-Socin H, Salenave S, Young J, Levasseur S, Assayag P, Beckers A, Chanson P. Long-term outcome of patients with acromegaly and congestive heart failure. J Clin Endocrinol Metab. 2004;89:5308–5313. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
