

Outcome of intracerebral hemorrhage associated with different oral anticoagulants
- PMID: 28381513
- PMCID: PMC5409844
- DOI: 10.1212/WNL.0000000000003886
Outcome of intracerebral hemorrhage associated with different oral anticoagulants
Erratum in
-
Outcome of intracerebral hemorrhage associated with different oral anticoagulants.Neurology. 2018 Jun 5;90(23):1084. doi: 10.1212/WNL.0000000000004976. Neurology. 2018. PMID: 29866942 Free PMC article. No abstract available.
Abstract
Objective: In an international collaborative multicenter pooled analysis, we compared mortality, functional outcome, intracerebral hemorrhage (ICH) volume, and hematoma expansion (HE) between non-vitamin K antagonist oral anticoagulation-related ICH (NOAC-ICH) and vitamin K antagonist-associated ICH (VKA-ICH).
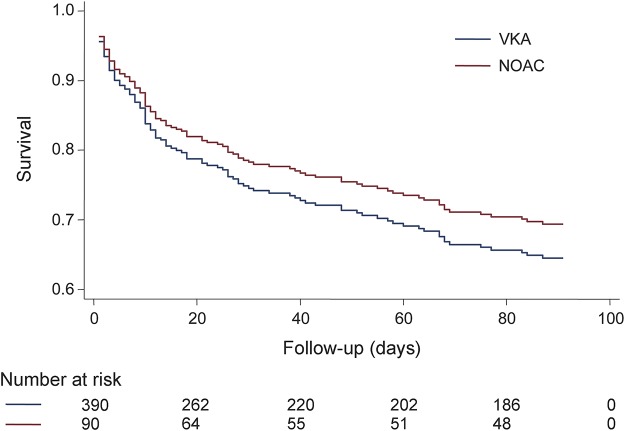
Methods: We compared all-cause mortality within 90 days for NOAC-ICH and VKA-ICH using a Cox proportional hazards model adjusted for age; sex; baseline Glasgow Coma Scale score, ICH location, and log volume; intraventricular hemorrhage volume; and intracranial surgery. We addressed heterogeneity using a shared frailty term. Good functional outcome was defined as discharge modified Rankin Scale score ≤2 and investigated in multivariable logistic regression. ICH volume was measured by ABC/2 or a semiautomated planimetric method. HE was defined as an ICH volume increase >33% or >6 mL from baseline within 72 hours.
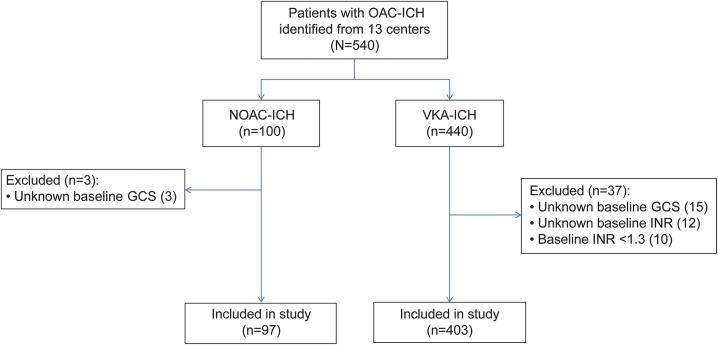
Results: We included 500 patients (97 NOAC-ICH and 403 VKA-ICH). Median baseline ICH volume was 14.4 mL (interquartile range [IQR] 3.6-38.4) for NOAC-ICH vs 10.6 mL (IQR 4.0-27.9) for VKA-ICH (p = 0.78). We did not find any difference between NOAC-ICH and VKA-ICH for all-cause mortality within 90 days (33% for NOAC-ICH vs 31% for VKA-ICH [p = 0.64]; adjusted Cox hazard ratio (for NOAC-ICH vs VKA-ICH) 0.93 [95% confidence interval (CI) 0.52-1.64] [p = 0.79]), the rate of HE (NOAC-ICH n = 29/48 [40%] vs VKA-ICH n = 93/140 [34%] [p = 0.45]), or functional outcome at hospital discharge (NOAC-ICH vs VKA-ICH odds ratio 0.47; 95% CI 0.18-1.19 [p = 0.11]).
Conclusions: In our international collaborative multicenter pooled analysis, baseline ICH volume, hematoma expansion, 90-day mortality, and functional outcome were similar following NOAC-ICH and VKA-ICH.
Copyright © 2017 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
The changing landscape of anticoagulant-related intracerebral hemorrhage.Neurology. 2017 May 2;88(18):1686-1687. doi: 10.1212/WNL.0000000000003895. Epub 2017 Apr 5. Neurology. 2017. PMID: 28381509 No abstract available.
References
-
- Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014;383:955–962. - PubMed
-
- Ansell J. New oral anticoagulants should not be used as first-line agents to prevent thromboembolism in patients with atrial fibrillation. Circulation 2012;125:165–170. - PubMed
-
- Schulman S, Majeed A. The oral thrombin inhibitor dabigatran: strengths and weaknesses. Semin Thromb Hemost 2012;38:7–15. - PubMed
-
- Purrucker JC, Haas K, Rizos T, et al. Early clinical and radiological course, management, and outcome of intracerebral hemorrhage related to new oral anticoagulants. JAMA Neurol 2016;73:169–177. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical