

Notable Increasing Trend in Azole Non-susceptible Candida tropicalis Causing Invasive Candidiasis in China (August 2009 to July 2014): Molecular Epidemiology and Clinical Azole Consumption
- PMID: 28382028
- PMCID: PMC5360734
- DOI: 10.3389/fmicb.2017.00464
Notable Increasing Trend in Azole Non-susceptible Candida tropicalis Causing Invasive Candidiasis in China (August 2009 to July 2014): Molecular Epidemiology and Clinical Azole Consumption
Abstract
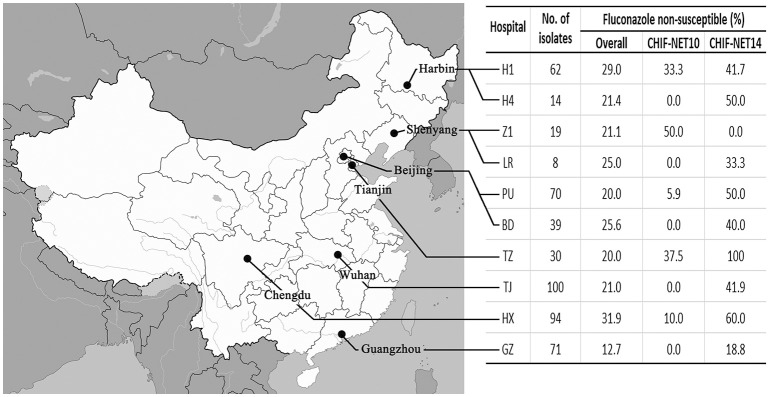
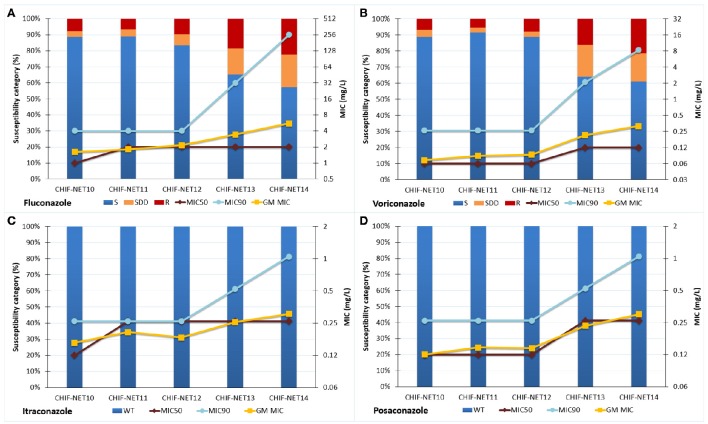
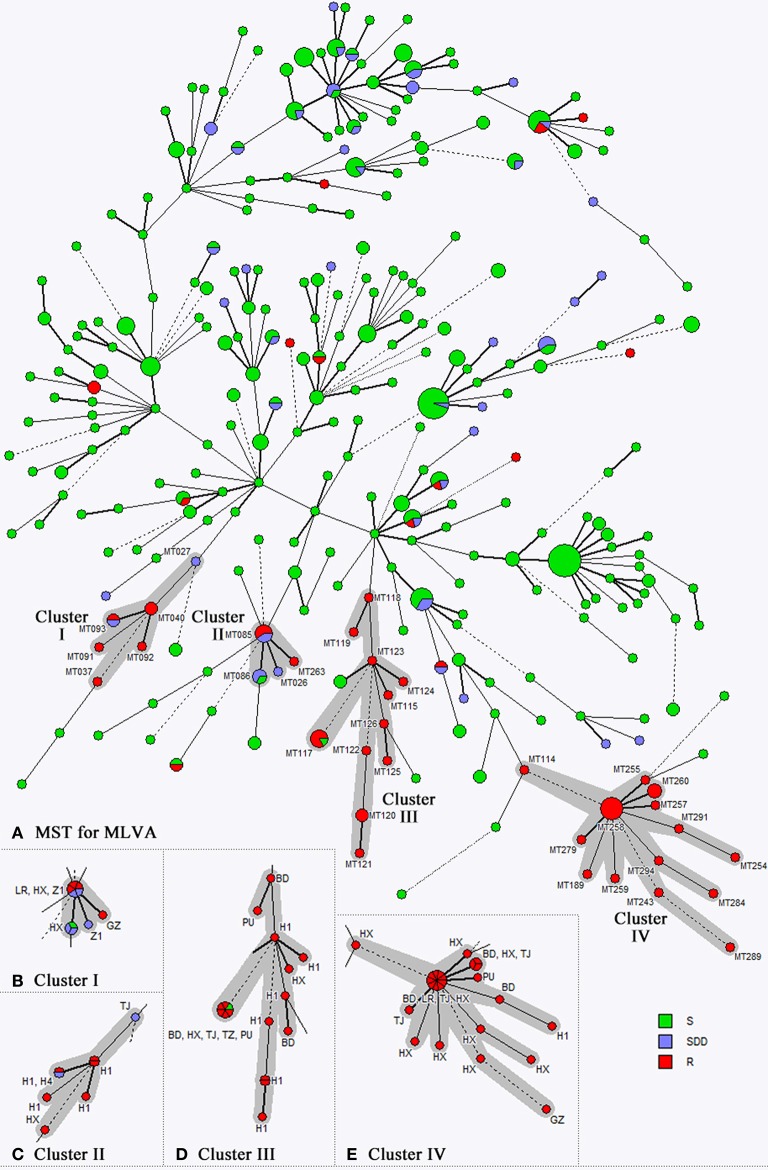
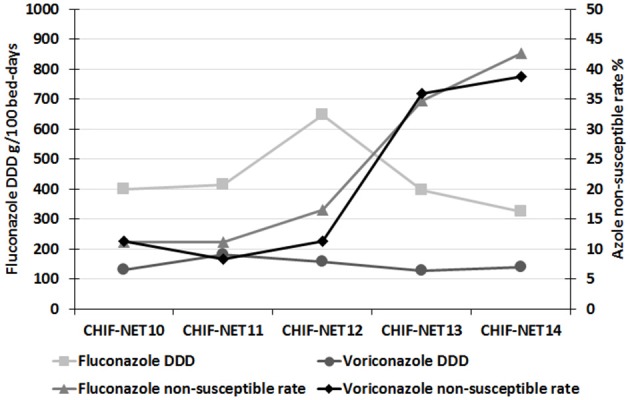
Objectives: To report the notable increasing trends of C. tropicalis antifungal resistance in the past 5 years, and explore molecular epidemiology, and the relationship between clinical azoles consumption and increased resistance rate. Methods: Between August 2009 and July 2014, 507 non-duplicated C. tropicalis isolates causing invasive candidiasis were collected from 10 hospitals in China. The in vitro antifungal susceptibility of nine common agents was determined by Sensititre YeastOne™ using current available species-specific clinical breakpoint (CBPs) or epidemiological cut-off values (ECVs). A high discriminatory three-locus (ctm1, ctm3, and ctm24) microsatellite scheme was used for typing of all isolates collected. Clinical consumption of fluconazole and voriconazole was obtained and the Defined Daily Dose measurement units were assigned to the data. Results: Overall, 23.1 and 20.7% of isolates were non-susceptible to fluconazole and voriconazole, respectively. And over 5 years, the non-susceptible rate of C. tropicalis isolates to fluconazole and voriconazole continuously increased from 11.2 to 42.7% for fluconazole (P < 0.001), and from 10.4 to 39.1% for voriconazole (P < 0.001). Four genotype clusters were observed to be associated with fluconazole non-susceptible phenotype. However, the increase in azole non-susceptible rate didn't correlate with clinical azole consumption. Conclusions: The rapid emergence of azole resistant C. tropicalis strains in China is worrying, and continuous surveillance is warranted and if the trend persists, empirical therapeutic strategies for C. tropicalis invasive infections should be modified.
Keywords: Candida tropicalis; China; antifungal susceptibility; azole resistance; genotyping; invasive candidiasis.
Figures
References
-
- Andes D. R., Safdar N., Baddley J. W., Alexander B., Brumble L., Freifeld A., et al. . (2016). The epidemiology and outcomes of invasive Candida infections among organ transplant recipients in the United States: results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Transpl. Infect. Dis. 18, 921–931. 10.1111/tid.12613 - DOI - PubMed
-
- Bordallo-Cardona M. A., Escribano P., de la Pedrosa E. G., Marcos-Zambrano L. J., Canton R., Bouza E., et al. . (2017). In vitro exposure to increasing micafungin concentrations easily promotes Echinocandin resistance in Candida glabrata isolates. Antimicrob. Agents Chemother. 61, e01542–e01516. 10.1128/AAC.01542-16 - DOI - PMC - PubMed
-
- Canton E., Peman J., Hervas D., Iniguez C., Navarro D., Echeverria J., et al. . (2012). Comparison of three statistical methods for establishing tentative wild-type population and epidemiological cutoff values for echinocandins, amphotericin B, flucytosine, and six Candida species as determined by the colorimetric Sensititre YeastOne method. J. Clin. Microbiol. 50, 3921–3926. 10.1128/JCM.01730-12 - DOI - PMC - PubMed
-
- Castanheira M., Messer S. A., Rhomberg P. R., Pfaller M. A. (2016). Antifungal susceptibility patterns of a global collection of fungal isolates: results of the SENTRY Antifungal Surveillance Program (2013). Diagn. Microbiol. Infect. Dis. 85, 200–204. 10.1016/j.diagmicrobio.2016.02.009 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous