

International multicenter comparative trial of endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for the treatment of malignant gastric outlet obstruction
- PMID: 28382326
- PMCID: PMC5378550
- DOI: 10.1055/s-0043-101695
International multicenter comparative trial of endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for the treatment of malignant gastric outlet obstruction
Abstract
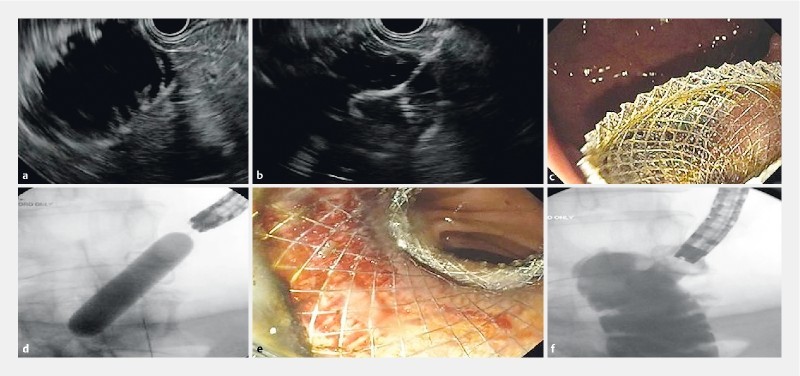
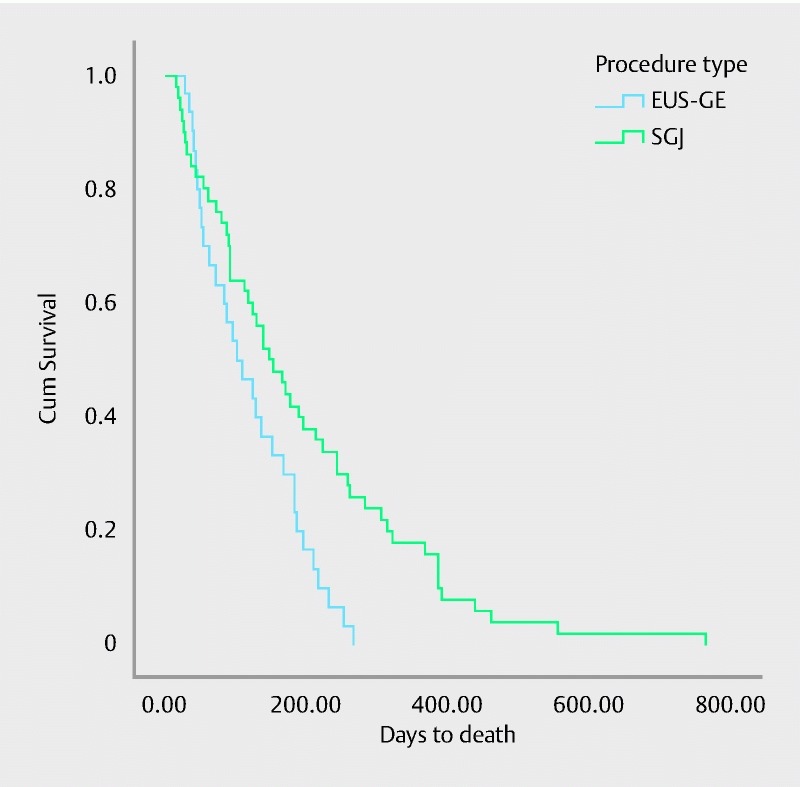
Background and study aims EUS-guided gastroenterostomy (EUS-GE) is a novel procedure that potentially offers long-lasting luminal patency without the risk of tumor ingrowth/overgrowth. This study compared the clinical success, technical success, adverse events (AEs), length of hospital stay (LOHS) and symptom recurrence in EUS-GE versus SGJ. Methods This was a multicenter international retrospective comparative study of EUS-GE and SGJ in patients with malignant gastric outlet obstruction (GOO) who underwent either EUS-GE or SGJ. EUS-GE was performed using lumen apposing metal stents. Results A total of 93 patients with malignant GOO treated with either EUS-GE (n = 30) or SGJ (n = 63) were identified. Peritoneal carcinomatosis was present in 13 (43 %) patients in the EUS-GE group and 7 (11 %) patients in the SGJ group (P < 0.001). Although the technical success rate was significantly higher in the SGJ group as compared to the EUS-GE group (100 % vs. 87 %, P = 0.009), the clinical success rate was not different (90 % vs. 87 %, P = 0.18, OR 0.8, 95 %CI 0.44 - 7.07). The rate of AEs was lower in the EUS-GE group, but the difference was not statistically significant (16 % vs 25 %, P = 0.3). The mean LOHS was similar in the EUS-GE group compared to SGJ (P = 0.35). The rate of recurrent GOO was not different between the two groups (3 % vs. 14 %, P = 0.08). Similarly, the mean time to reintervention was similar (88 days vs. 121 days, P = 0.83). Conclusions EUS-GE is associated with equivalent efficacy and safety as compared to surgical GJ. This is the first comparative trial between both techniques and suggests EUS-GE as a non-inferior but less invasive alter to surgery.
Conflict of interest statement
Figures
References
-
- van Heek N T, van Geenen R C, Busch O R et al.Palliative treatment in “peri”-pancreatic carcinoma: stenting or surgical therapy? Acta Gastro-enterologica Belgica. 2002;65:171–175. - PubMed
-
- van Hooft J E, Uitdehaag M J, Bruno M J et al.Efficacy and safety of the new WallFlex enteral stent in palliative treatment of malignant gastric outlet obstruction (DUOFLEX study): a prospective multicenter study. Gastrointest Endosc. 2009;69:1059–1066. - PubMed
-
- Johnsson E, Thune A, Liedman B. Palliation of malignant gastroduodenal obstruction with open surgical bypass or endoscopic stenting: clinical outcome and health economic evaluation. World J Surgery. 2004;28:812–817. - PubMed
-
- Mehta S, Hindmarsh A, Cheong E et al.Prospective randomized trial of laparoscopic gastrojejunostomy versus duodenal stenting for malignant gastric outflow obstruction. Surg Endosc. 2006;20:239–242. - PubMed
-
- Fiori E, Lamazza A, Volpino P et al.Palliative management of malignant antro-pyloric strictures. Gastroenterostomy vs. endoscopic stenting. A randomized prospective trial. Anticancer Res. 2004;24:269–271. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical