

Pseudoprogression, radionecrosis, inflammation or true tumor progression? challenges associated with glioblastoma response assessment in an evolving therapeutic landscape
- PMID: 28382534
- PMCID: PMC7893814
- DOI: 10.1007/s11060-017-2375-2
Pseudoprogression, radionecrosis, inflammation or true tumor progression? challenges associated with glioblastoma response assessment in an evolving therapeutic landscape
Abstract
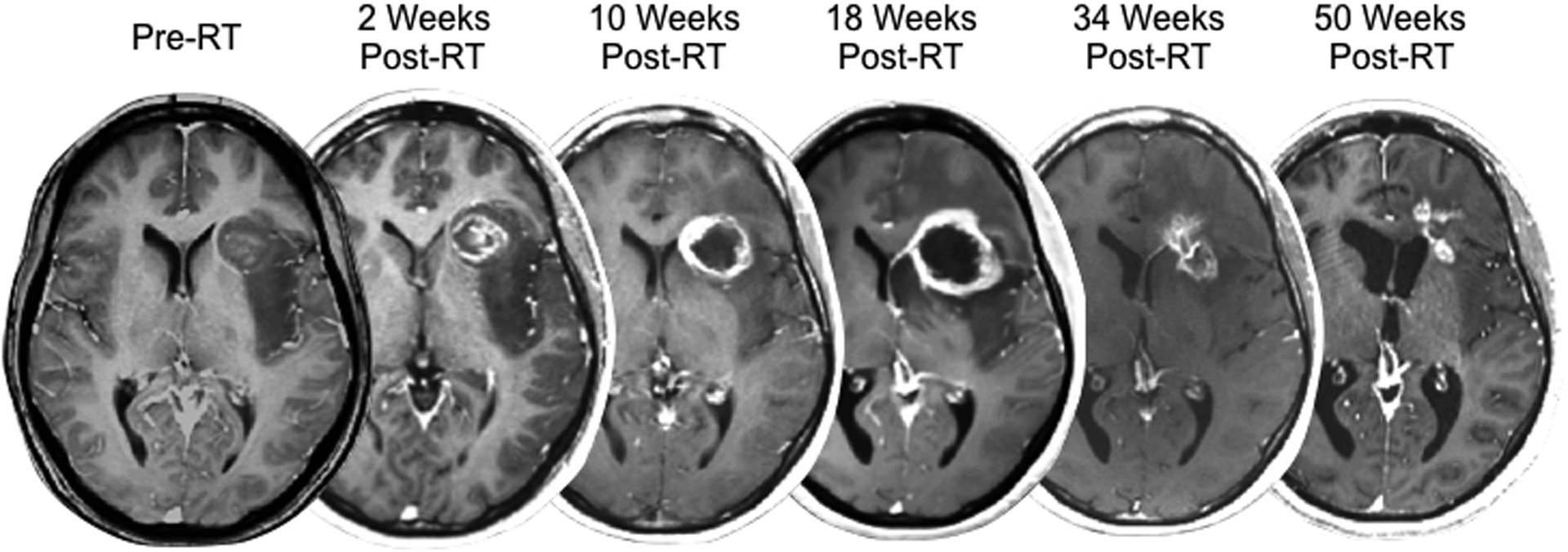
The wide variety of treatment options that exist for glioblastoma, including surgery, ionizing radiation, anti-neoplastic chemotherapies, anti-angiogenic therapies, and active or passive immunotherapies, all may alter aspects of vascular permeability within the tumor and/or normal parenchyma. These alterations manifest as changes in the degree of contrast enhancement or T2-weighted signal hyperintensity on standard anatomic MRI scans, posing a potential challenge for accurate radiographic response assessment for identifying anti-tumor effects. The current review highlights the challenges that remain in differentiating true disease progression from changes due to radiation therapy, including pseudoprogression and radionecrosis, as well as immune or inflammatory changes that may occur as either an undesired result of cytotoxic therapy or as a desired consequence of immunotherapies.
Keywords: Glioblastoma; Imaging; Pseudoprogression; Radiation necrosis.
Figures
References
-
- Leon SP, Folkerth RD, Black PM: Microvessel density is a prognostic indicator for patients with astroglial brain tumors. Cancer 77: 362–372, 1996 - PubMed
-
- Wesseling P, van der Laak JA, Link M, Teepen HL, Ruiter DJ: Quantitative analysis of microvascular changes in diffuse astrocytic neoplasms with increasing grade of malignancy. Hum Pathol 29: 352–358, 1998 - PubMed
-
- Folkman J: Role of angiogenesis in tumor growth and metastasis. Semin Oncol 29: 15–18, 2002 - PubMed
-
- Kelly PJ, Daumas-Duport C, Kispert DB, Kall BA, Scheithauer BW, Illig JJ: Imaging-based stereotaxic serial biopsies in untreated intracranial glial neoplasms. J Neurosurg 66: 865–874, 1987 - PubMed
-
- Macdonald DR, Cascino TL, Schold SC Jr., Cairncross JG: Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol 8: 1277–1280, 1990 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
