

Creating an automated trigger for sepsis clinical decision support at emergency department triage using machine learning
- PMID: 28384212
- PMCID: PMC5383046
- DOI: 10.1371/journal.pone.0174708
Creating an automated trigger for sepsis clinical decision support at emergency department triage using machine learning
Abstract
Objective: To demonstrate the incremental benefit of using free text data in addition to vital sign and demographic data to identify patients with suspected infection in the emergency department.
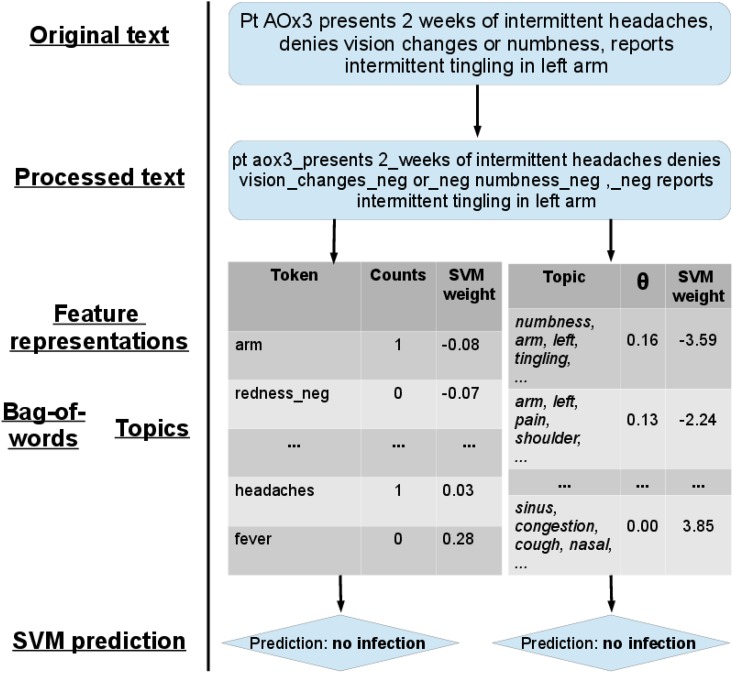
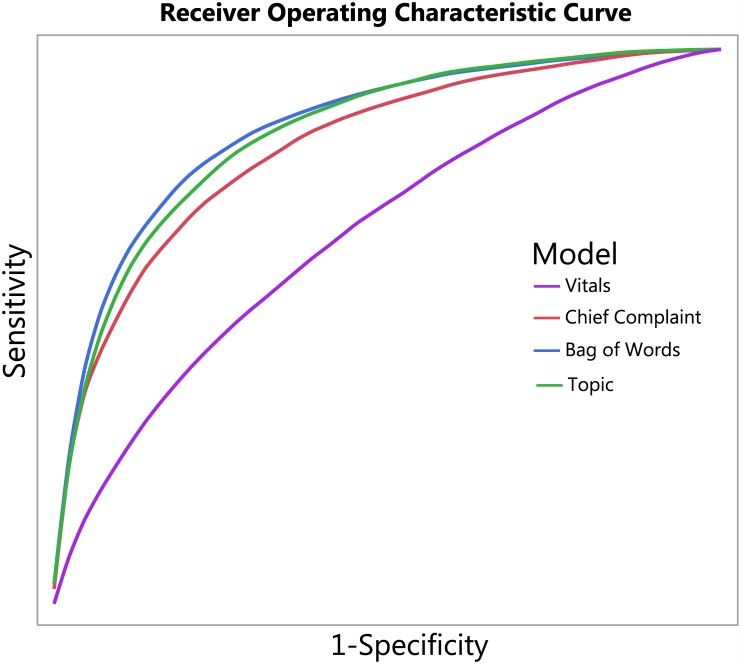
Methods: This was a retrospective, observational cohort study performed at a tertiary academic teaching hospital. All consecutive ED patient visits between 12/17/08 and 2/17/13 were included. No patients were excluded. The primary outcome measure was infection diagnosed in the emergency department defined as a patient having an infection related ED ICD-9-CM discharge diagnosis. Patients were randomly allocated to train (64%), validate (20%), and test (16%) data sets. After preprocessing the free text using bigram and negation detection, we built four models to predict infection, incrementally adding vital signs, chief complaint, and free text nursing assessment. We used two different methods to represent free text: a bag of words model and a topic model. We then used a support vector machine to build the prediction model. We calculated the area under the receiver operating characteristic curve to compare the discriminatory power of each model.
Results: A total of 230,936 patient visits were included in the study. Approximately 14% of patients had the primary outcome of diagnosed infection. The area under the ROC curve (AUC) for the vitals model, which used only vital signs and demographic data, was 0.67 for the training data set, 0.67 for the validation data set, and 0.67 (95% CI 0.65-0.69) for the test data set. The AUC for the chief complaint model which also included demographic and vital sign data was 0.84 for the training data set, 0.83 for the validation data set, and 0.83 (95% CI 0.81-0.84) for the test data set. The best performing methods made use of all of the free text. In particular, the AUC for the bag-of-words model was 0.89 for training data set, 0.86 for the validation data set, and 0.86 (95% CI 0.85-0.87) for the test data set. The AUC for the topic model was 0.86 for the training data set, 0.86 for the validation data set, and 0.85 (95% CI 0.84-0.86) for the test data set.
Conclusion: Compared to previous work that only used structured data such as vital signs and demographic information, utilizing free text drastically improves the discriminatory ability (increase in AUC from 0.67 to 0.86) of identifying infection.
Conflict of interest statement
Figures
References
-
- Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, et al. (2006) Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med 144: 742–752. - PubMed
-
- Institute of Medicine (U.S.). Committee on the Future of Emergency Care in the United States Health System. (2007) Hospital-based emergency care: at the breaking point. Washington, D.C.: National Academies Press; xxiii, 397 p. p.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
