

Impact of genotype and phenotype on cardiac biomarkers in patients with transthyretin amyloidosis - Report from the Transthyretin Amyloidosis Outcome Survey (THAOS)
- PMID: 28384285
- PMCID: PMC5383030
- DOI: 10.1371/journal.pone.0173086
Impact of genotype and phenotype on cardiac biomarkers in patients with transthyretin amyloidosis - Report from the Transthyretin Amyloidosis Outcome Survey (THAOS)
Abstract
Aim: Cardiac troponins and natriuretic peptides are established for risk stratification in light-chain amyloidosis. Data on cardiac biomarkers in transthyretin amyloidosis (ATTR) are lacking.
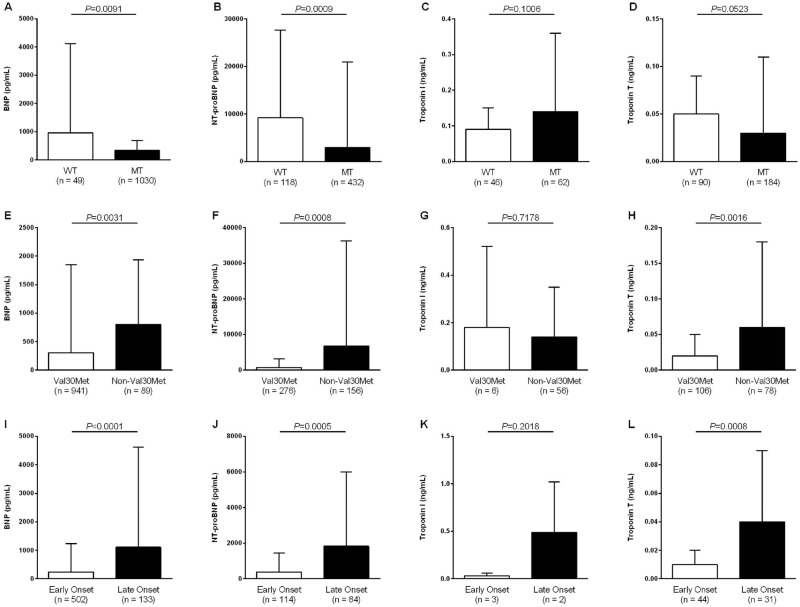
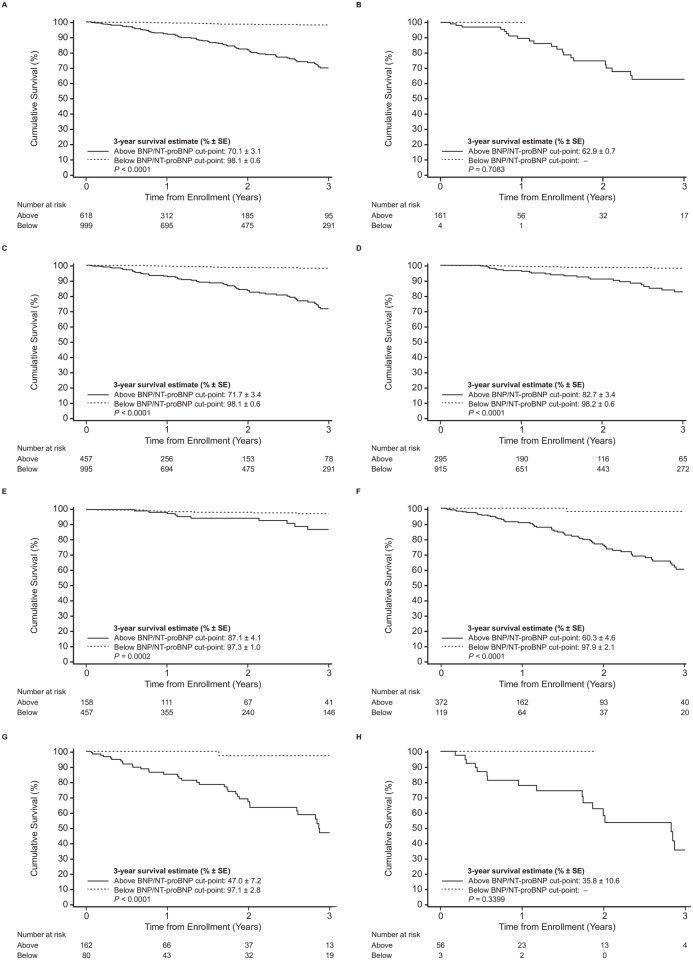
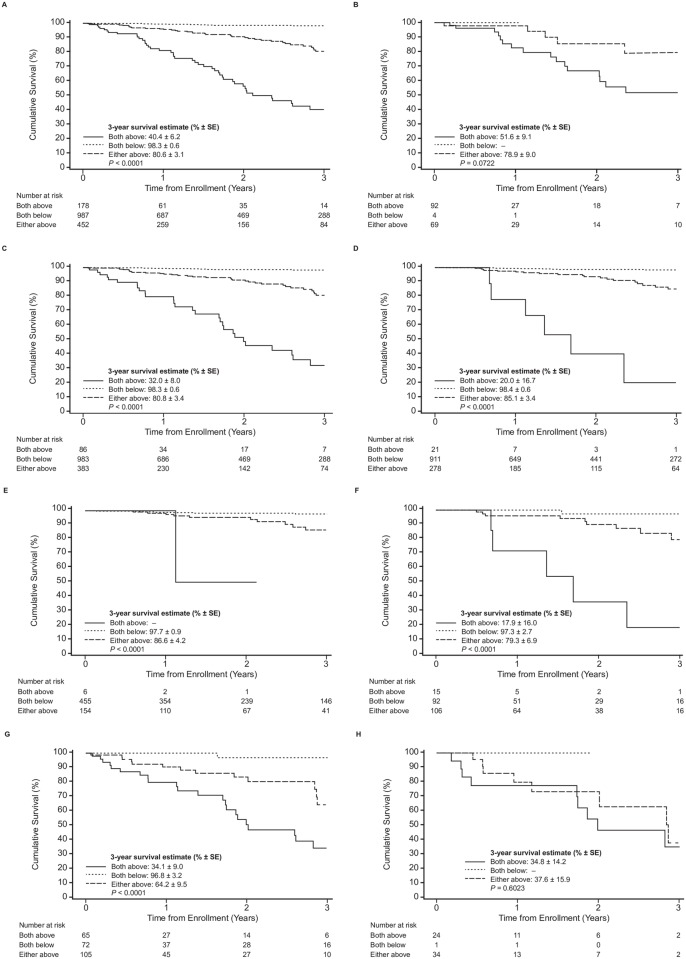
Methods and results: Patients (n = 1617) with any of the following cardiac biomarkers, BNP (n = 1079), NT-proBNP (n = 550), troponin T (n = 274), and troponin I (n = 108), available at baseline in the Transthyretin Amyloidosis Outcomes Survey (THAOS) were analyzed for differences between genotypes and phenotypes and their association with survival. Median level of BNP was 68.0 pg/mL (IQR 30.5-194.9), NT-proBNP 337.9 pg/mL (IQR 73.0-2584.0), troponin T 0.03 μg/L (IQR 0.01-0.05), and troponin I 0.08 μg/L (IQR 0.04-0.13). NT-proBNP and BNP were higher in wild-type than mutant-type ATTR, troponin T and I did not differ, respectively. Non-Val30Met patients had higher BNP, NT-proBNP and troponin T levels than Val30Met patients, but not troponin I. Late-onset Val30Met was associated with higher levels of troponin I and troponin T compared with early-onset. 115 patients died during a median follow-up of 1.2 years. Mortality increased with increasing quartiles (BNP/NT-proBNP Q1 = 1.7%, Q2 = 5.2%, Q3 = 21.7%, Q4 = 71.3%; troponin T/I Q1 = 6.5%, Q2 = 14.5%, Q3 = 33.9%, Q4 = 45.2%). Three-year overall-survival estimates for BNP/NT-proBNP and troponin T/I quartiles differed significantly (p<0.001). Stepwise risk stratification was achieved by combining NT-proBNP/BNP and troponin T/I. From Cox proportional hazards model, age, modified body mass index, mutation (Val30Met vs. Non-Val30Met) and BNP/NT-proBNP (Q1-Q3 pooled vs. Q4) were identified as independent predictors of survival in patients with mutant-type ATTR.
Conclusions: In this ATTR patient cohort, cardiac biomarkers were abnormal in a substantial percentage of patients irrespective of genotype. Along with age, mBMI, and mutation (Val30Met vs. Non-Val30Met), cardiac biomarkers were associated with surrogates of disease severity with BNP/NT-proBNP identified as an independent predictor of survival in ATTR.
Trial registration: ClinicalTrials.gov NCT00628745.
Conflict of interest statement
Figures
References
-
- Benson MD (2012) Pathogenesis of transthyretin amyloidosis. Amyloid 19 Suppl 1: 14–15. - PubMed
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
