

Repeated lumbar or ventricular punctures in newborns with intraventricular haemorrhage
- PMID: 28384379
- PMCID: PMC6478098
- DOI: 10.1002/14651858.CD000216.pub2
Repeated lumbar or ventricular punctures in newborns with intraventricular haemorrhage
Abstract
Background: Although in recent years the percentage of preterm infants who suffer intraventricular haemorrhage (IVH) has reduced, posthaemorrhagic hydrocephalus (PHH) remains a serious problem with a high rate of cerebral palsy and no evidence-based treatment. Survivors often have to undergo ventriculoperitoneal shunt (VPS) surgery, which makes the child permanently dependent on a valve and catheter system. This carries a significant risk of infection and the need for surgical revision of the shunt. Repeated removal of cerebrospinal fluid (CSF) by either lumbar puncture, ventricular puncture, or from a ventricular reservoir in preterm babies with IVH has been suggested as a treatment to reduce the risk of PHH development.
Objectives: To determine the effect of repeated cerebrospinal fluid (CSF) removal (by lumbar/ventricular puncture or removal from a ventricular reservoir) compared to conservative management, where removal is limited to when there are signs of raised intracranial pressure (ICP), on reduction in the risk of permanent shunt dependence, neurodevelopmental disability, and death in neonates with or at risk of developing posthaemorrhagic hydrocephalus (PHH).
Search methods: We used the standard search strategy of Cochrane Neonatal to search the Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue 3), MEDLINE via PubMed (1966 to 24 March 2016), Embase (1980 to 24 March 2016), and CINAHL (1982 to 24 March 2016). We also searched clinical trials databases, conference proceedings, and the reference lists of retrieved articles for randomised controlled trials (RCTs) and quasi-RCTs.
Selection criteria: RCTs and quasi-RCTs that compared serial removal of CSF (via lumbar puncture, ventricular puncture, or from a ventricular reservoir) with conservative management (removing CSF only when there were symptoms of raised ICP). Trials also had to report on at least one of the specified outcomes of death, disability, or shunt insertion.
Data collection and analysis: We extracted details of the participant selection, participant allocation and the interventions. We assessed the following outcomes: VPS, death, death or shunt, disability, multiple disability, death or disability, and CSF infection. We assessed the quality of the evidence using the GRADE approach.
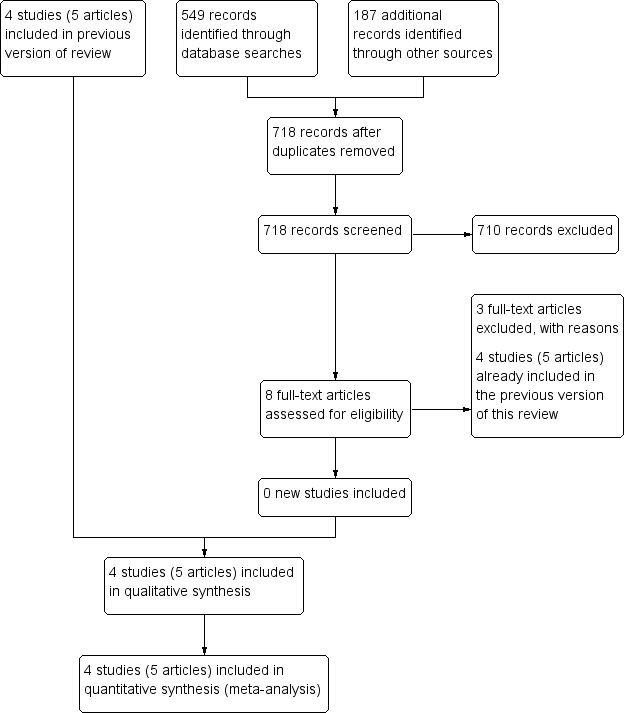
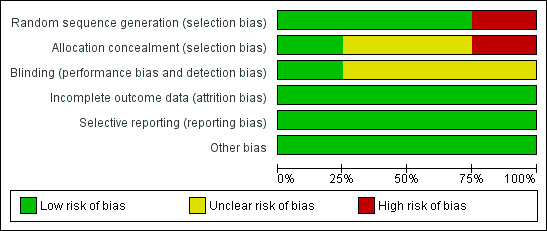
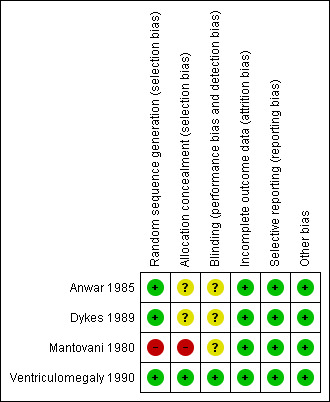
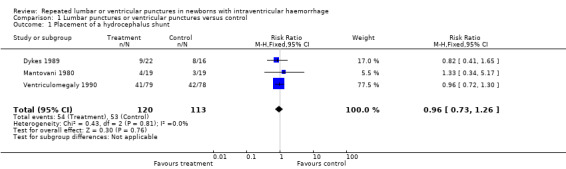
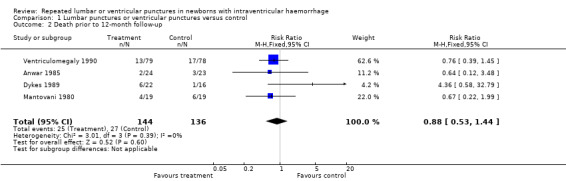
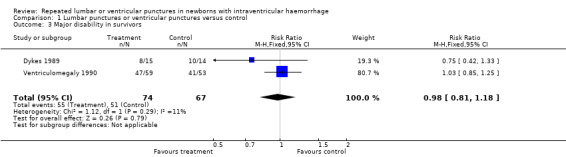
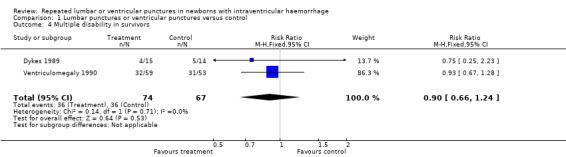
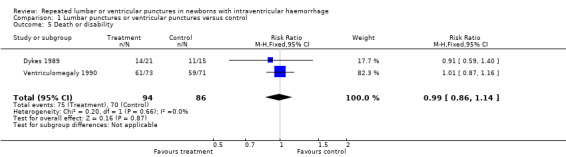
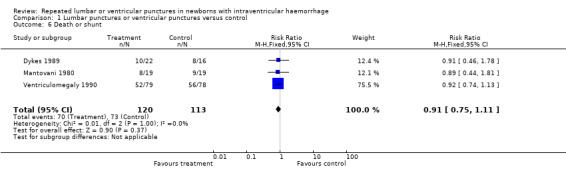
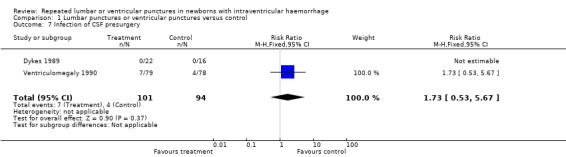
Main results: Four trials (five articles) met the inclusion criteria of this review; three were RCTs and one was a quasi-RCT; and included a total of 280 participants treated in neonatal intensive care units in the UK. The trials were published between 1980 and 1990. The studies were sufficiently similar regarding the research question they asked and the interventions that we could combine the trials to assess the effect of the intervention.Meta-analysis showed that the intervention produced no significant difference when compared to conservative management for the outcomes of: placement of hydrocephalus shunt (typical risk ratio (RR) 0.96, 95% confidence interval (CI) 0.73 to 1.26; 3 trials, 233 infants; I² statistic = 0%; moderate quality evidence), death (RR 0.88, 95% CI 0.53 to 1.44; 4 trials, 280 infants; I² statistic = 0%; low quality evidence), major disability in survivors (RR 0.98, 95% CI 0.81 to 1.18; 2 trials, 141 infants; I² statistic = 11%; high quality evidence), multiple disability in survivors (RR 0.9, 95% CI 0.66 to 1.24; 2 trials, 141 infants; I² statistic = 0%; high quality evidence), death or disability (RR 0.99, 95% CI 0.86 to 1.14; 2 trials, 180 infants; I² statistic = 0%; high quality evidence), death or shunt (RR 0.91, 95% CI 0.75 to 1.11; 3 trials, 233 infants; I² statistic = 0%; moderate quality evidence), and infection of CSF presurgery (RR 1.73, 95% CI 0.53 to 5.67; 2 trials, 195 infants; low quality evidence).We assessed the quality of the evidence as high for the outcomes of major disability, multiple disability, and disability or death. We rated the evidence for the outcomes of shunt insertion, and death or shunt insertion as of moderate quality as one included trial used an alternation method of randomisation. For the outcomes of death and infection of CSF presurgery, the quality of the evidence was low as one trial used an alternation method, the number of participants was too low to assess the objectives with sufficient precision, and there was inconsistency regarding the findings in the included trials regarding the outcome of infection of CSF presurgery.
Authors' conclusions: There was no evidence that repeated removal of CSF via lumbar puncture, ventricular puncture or from a ventricular reservoir produces any benefit over conservative management in neonates with or at risk for developing PHH in terms of reduction of disability, death, or need for placement of a permanent shunt.
Conflict of interest statement
AW is an author of one of the included trials (Ventriculomegaly 1990). RLK has no known conflicts of interest.
Figures
Update of
-
Repeated lumbar or ventricular punctures in newborns with intraventricular hemorrhage.Cochrane Database Syst Rev. 2001;(1):CD000216. doi: 10.1002/14651858.CD000216. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2017 Apr 06;4:CD000216. doi: 10.1002/14651858.CD000216.pub2. PMID: 11279684 Updated.
References
References to studies included in this review
Anwar 1985 {published data only}
-
- Anwar M, Kadam S, Hiatt IM, Hegyi T. Serial lumbar punctures in prevention of post‐hemorrhagic hydrocephalus in preterm infants. Journal of Pediatrics 1985;107(3):446‐50. - PubMed
Dykes 1989 {published data only}
-
- Dykes FD, Dunbar B, Lazarra A, Ahmann PA. Posthemorrhagic hydrocephalus in high risk infants: Natural history, management, and long‐term outcome. Journal of Pediatrics 1989;114(4 Pt 1):611‐8. - PubMed
Mantovani 1980 {published data only}
-
- Mantovani JF, Pasternak JF, Mathew OP, Allen WC, Mills MT, Casper J, et al. Failure of daily lumbar punctures to prevent the development of hydrocephalus following intraventricular hemorrhage. Journal of Pediatrics 1980;97(2):278‐81. - PubMed
Ventriculomegaly 1990 {published data only}
References to studies excluded from this review
Kreusser 1985 {published data only}
-
- Kreusser KL, Tarby TJ, Kovnar E, Taylor DA, Hill A, Volpe JJ. Serial lumbar punctures for at least temporary amelioration of neonatal posthemorrhagic hydrocephalus. Pediatrics 1985;75(4):719‐24. - PubMed
Lipscomb 1983 {published data only}
-
- Lipscomb A, Thorburn R, Stewart AL, Reynolds EO, Hope PL. Early treatment for rapidly progressive posthaemorrhagic hydrocephalus. Lancet 1983;1(8339):1438‐9. - PubMed
Papile 1980 {published data only}
-
- Papile LA, Burstein J, Burstein R, Koffler H, Koops BL, Johnson JD. Posthemorrhagic hydrocephalus in low‐birth‐weight infants: treatment by serial lumbar punctures. Journal of Pediatrics 1980;97(2):273‐7. - PubMed
References to ongoing studies
ISRCTN43171322 {published data only}
-
- ISRCTN43171322. A multicentre randomised controlled trial of low versus high threshold treatment in preterm infants with progressive posthaemorrhagic ventricular dilatation (PHVD). http://www.isrctn.com/ISRCTN43171322 (first received 27 January 2006). [DOI: 10.1186/ISRCTN43171322] - DOI
Additional references
Bassan 2012
-
- Bassan H, Eshel R, Golan I, Kohelet D, Ben Sira L, Mandel D, et al. Timing of external ventricular drainage and neurodevelopmental outcome in preterm infants with posthemorrhagic hydrocephalus. European Journal of Paediatric Neurology 2012;16(6):662‐70. - PubMed
Cherian 2004
de Vries 2002
-
- Vries LS, Liem KD, Dijk K, Smit BJ, Sie L, Rademaker KJ, et al. Early versus late treatment of posthaemorrhagic ventricular dilatation: results of a retrospective study from five neonatal intensive care units in The Netherlands. Acta Paediatrica 2002;91(2):212‐7. - PubMed
GRADEpro GDT 2014 [Computer program]
-
- GRADE Working Group, McMaster University. GRADEpro [www.gradepro.org]. Version accessed 24 March 2016. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Hislop 1988
-
- Hislop JE, Dubowitz LM, Kaiser AM, Singh MP, Whitelaw AG. Outcome of infants shunted for post‐haemorrhagic ventricular dilatation. Developmental Medicine and Child Neurology 1988;30(4):451‐6. - PubMed
Klebermass‐Schrehof 2013
-
- Klebermass‐Schrehof K, Rona Z, Waldhör T, Czaba C, Beke A, Weninger M, et al. Can neurophysiological assessment improve timing of intervention in posthaemorrhagic ventricular dilatation?. Archives of Disease in Childhood. Fetal and Neonatal Edition 2013;98(4):F291‐7. - PubMed
Levene 1981
Olischar 2009
-
- Olischar M, Klebermass K, Hengl B, Hunt RW, Waldhoer T, Pollak A, et al. Cerebrospinal fluid drainage in posthaemorrhagic ventricular dilatation leads to improvement in amplitude‐integrated electroencephalographic activity. Acta Paediatrica 2009;98(6):1002‐9. - PubMed
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Savman 2001
-
- Savman K, Nilsson UA, Blennow M, Kjellmer I, Whitelaw A. Non‐protein‐bound iron is elevated in cerebrospinal fluid from preterm infants with posthemorrhagic ventricular dilatation. Pediatric Research 2001;49(2):208‐12. - PubMed
Schünemann 2013
-
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE Working Group. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. Available from www.guidelinedevelopment.org/handbook (accessed 24 March 2016).
Sävman 2002
-
- Sävman K, Blennow M, Hagberg H, Tarkowski E, Thoresen M, Whitelaw A. Cytokine response in cerebrospinal fluid from preterm infants with posthaemorrhagic ventricular dilatation. Acta Paediatrica 2002;91(12):1357‐63. - PubMed
Taylor 2001
-
- Taylor AG, Peter JC. Advantages of delayed VP shunting in post‐haemorrhagic hydrocephalus seen in low‐birth‐weight infants. Child's Nervous System 2001;17(6):328‐33. - PubMed
Tuli 2003
-
- Tuli S, Drake J, Lamberti‐Pasculli M. Long‐term outcome of hydrocephalus management in myelomeningoceles. Child's Nervous System 2003;19(5‐6):286‐91. - PubMed
Whitelaw 2001b
Whitelaw 2007
Whitelaw 2010
-
- Whitelaw A, Jary S, Kmita G, Wroblewska J, Musialik‐Swietlinska E, Mandera M, et al. Randomized trial of drainage, irrigation and fibrinolytic therapy for premature infants with posthemorrhagic ventricular dilatation: developmental outcome at 2 years. Pediatrics 2010;125(4):e852‐8. - PubMed
References to other published versions of this review
Whitelaw 1998
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous