

Clinical Characterization of the Pheochromocytoma and Paraganglioma Susceptibility Genes SDHA, TMEM127, MAX, and SDHAF2 for Gene-Informed Prevention
- PMID: 28384794
- PMCID: PMC5824290
- DOI: 10.1001/jamaoncol.2017.0223
Clinical Characterization of the Pheochromocytoma and Paraganglioma Susceptibility Genes SDHA, TMEM127, MAX, and SDHAF2 for Gene-Informed Prevention
Abstract
Importance: Effective cancer prevention is based on accurate molecular diagnosis and results of genetic family screening, genotype-informed risk assessment, and tailored strategies for early diagnosis. The expanding etiology for hereditary pheochromocytomas and paragangliomas has recently included SDHA, TMEM127, MAX, and SDHAF2 as susceptibility genes. Clinical management guidelines for patients with germline mutations in these 4 newly included genes are lacking.
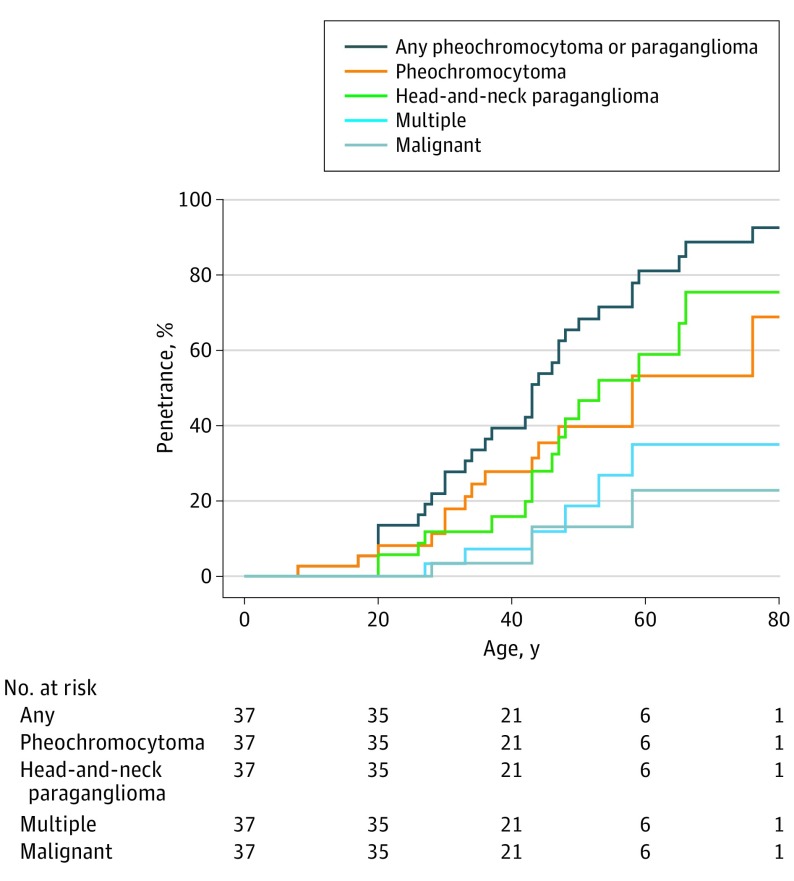
Objective: To study the clinical spectra and age-related penetrance of individuals with mutations in the SDHA, TMEM127, MAX, and SDHAF2 genes.
Design, setting, and patients: This study analyzed the prospective, longitudinally followed up European-American-Asian Pheochromocytoma-Paraganglioma Registry for prevalence of SDHA, TMEM127, MAX, and SDHAF2 germline mutation carriers from 1993 to 2016. Genetic predictive testing and clinical investigation by imaging from neck to pelvis was offered to mutation-positive registrants and their relatives to clinically characterize the pheochromocytoma/paraganglioma diseases associated with mutations of the 4 new genes.
Main outcomes and measures: Prevalence and spectra of germline mutations in the SDHA, TMEM127, MAX, and SDHAF2 genes were assessed. The clinical features of SDHA, TMEM127, MAX, and SDHAF2 disease were characterized.
Results: Of 972 unrelated registrants without mutations in the classic pheochromocytoma- and paraganglioma-associated genes (632 female [65.0%] and 340 male [35.0%]; age range, 8-80; mean [SD] age, 41.0 [13.3] years), 58 (6.0%) carried germline mutations of interest, including 29 SDHA, 20 TMEM127, 8 MAX, and 1 SDHAF2. Fifty-three of 58 patients (91%) had familial, multiple, extra-adrenal, and/or malignant tumors and/or were younger than 40 years. Newly uncovered are 7 of 63 (11%) malignant pheochromocytomas and paragangliomas in SDHA and TMEM127 disease. SDHA disease occurred as early as 8 years of age. Extra-adrenal tumors occurred in 28 mutation carriers (48%) and in 23 of 29 SDHA mutation carriers (79%), particularly with head and neck paraganglioma. MAX disease occurred almost exclusively in the adrenal glands with frequently bilateral tumors. Penetrance in the largest subset, SDHA carriers, was 39% at 40 years of age and is statistically different in index patients (45%) vs mutation-carrying relatives (13%; P < .001).
Conclusions and relevance: The SDHA, TMEM127, MAX, and SDHAF2 genes may contribute to hereditary pheochromocytoma and paraganglioma. Genetic testing is recommended in patients at clinically high risk if the classic genes are mutation negative. Gene-specific prevention and/or early detection requires regular, systematic whole-body investigation.
Conflict of interest statement
Figures

Comment in
-
Pheochromocytoma and Paraganglioma Susceptibility Genes: Estimating the Associated Risk of Disease.JAMA Oncol. 2017 Sep 1;3(9):1212-1213. doi: 10.1001/jamaoncol.2017.0222. JAMA Oncol. 2017. PMID: 28384677 No abstract available.
References
-
- Amar L, Bertherat J, Baudin E, et al. Genetic testing in pheochromocytoma or functional paraganglioma. J Clin Oncol. 2005;23(34):8812-8818. - PubMed
-
- Bausch B, Borozdin W, Neumann HP; European-American Pheochromocytoma Study Group . Clinical and genetic characteristics of patients with neurofibromatosis type 1 and pheochromocytoma. N Engl J Med. 2006;354(25):2729-2731. - PubMed
-
- Benn DE, Gimenez-Roqueplo AP, Reilly JR, et al. Clinical presentation and penetrance of pheochromocytoma/paraganglioma syndromes. J Clin Endocrinol Metab. 2006;91(3):827-836. - PubMed
-
- Jafri M, Whitworth J, Rattenberry E, et al. Evaluation of SDHB, SDHD and VHL gene susceptibility testing in the assessment of individuals with non-syndromic phaeochromocytoma, paraganglioma and head and neck paraganglioma. Clin Endocrinol (Oxf). 2013;78(6):898-906. - PubMed
-
- Mannelli M, Castellano M, Schiavi F, et al. ; Italian Pheochromocytoma/Paraganglioma Network . Clinically guided genetic screening in a large cohort of Italian patients with pheochromocytomas and/or functional or nonfunctional paragangliomas. J Clin Endocrinol Metab. 2009;94(5):1541-1547. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
