

The "surprise question" for predicting death in seriously ill patients: a systematic review and meta-analysis
- PMID: 28385893
- PMCID: PMC5378508
- DOI: 10.1503/cmaj.160775
The "surprise question" for predicting death in seriously ill patients: a systematic review and meta-analysis
Abstract
Background: The surprise question - "Would I be surprised if this patient died in the next 12 months?" - has been used to identify patients at high risk of death who might benefit from palliative care services. Our objective was to systematically review the performance characteristics of the surprise question in predicting death.
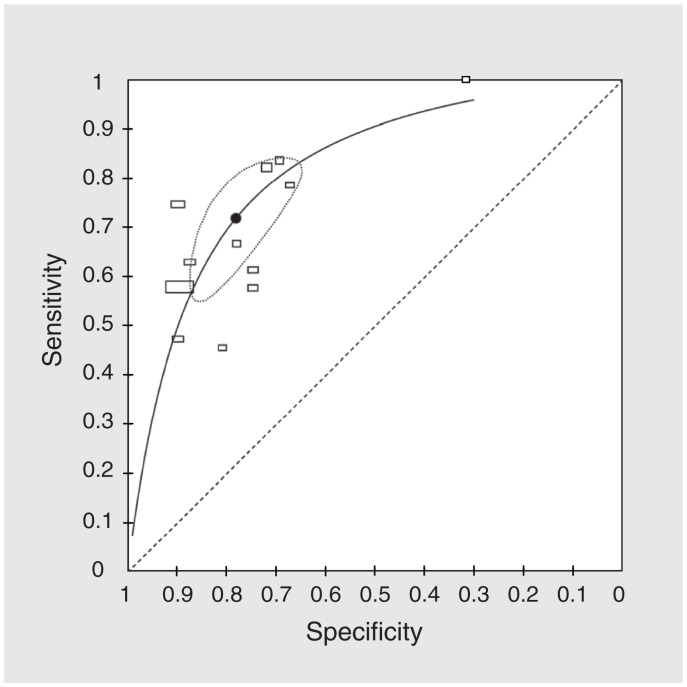
Methods: We searched multiple electronic databases from inception to 2016 to identify studies that prospectively screened patients with the surprise question and reported on death at 6 to 18 months. We constructed models of hierarchical summary receiver operating characteristics (sROCs) to determine prognostic performance.
Results: Sixteen studies (17 cohorts, 11 621 patients) met the selection criteria. For the outcome of death at 6 to 18 months, the pooled prognostic characteristics were sensitivity 67.0% (95% confidence interval [CI] 55.7%-76.7%), specificity 80.2% (73.3%-85.6%), positive likelihood ratio 3.4 (95% CI 2.8-4.1), negative likelihood ratio 0.41 (95% CI 0.32-0.54), positive predictive value 37.1% (95% CI 30.2%-44.6%) and negative predictive value 93.1% (95% CI 91.0%-94.8%). The surprise question had worse discrimination in patients with noncancer illness (area under sROC curve 0.77 [95% CI 0.73-0.81]) than in patients with cancer (area under sROC curve 0.83 [95% CI 0.79-0.87; p = 0.02 for difference]). Most studies had a moderate to high risk of bias, often because they had a low or unknown participation rate or had missing data.
Interpretation: The surprise question performs poorly to modestly as a predictive tool for death, with worse performance in noncancer illness. Further studies are needed to develop accurate tools to identify patients with palliative care needs and to assess the surprise question for this purpose.
© 2017 Canadian Medical Association or its licensors.
Figures

Comment in
-
About the "surprise question".CMAJ. 2017 Jun 12;189(23):E807. doi: 10.1503/cmaj.733083. CMAJ. 2017. PMID: 28606980 Free PMC article. No abstract available.
-
Response to: "About the 'surprise question'".CMAJ. 2017 Jun 12;189(23):E808. doi: 10.1503/cmaj.733094. CMAJ. 2017. PMID: 28606981 Free PMC article. No abstract available.
-
The utility and value of the "surprise question" for patients with serious illness.CMAJ. 2017 Aug 21;189(33):E1072-E1073. doi: 10.1503/cmaj.733231. CMAJ. 2017. PMID: 28827439 Free PMC article. No abstract available.
-
The authors respond to "The utility and value of the 'surprise question' for patients with serious illness".CMAJ. 2017 Aug 21;189(33):E1074. doi: 10.1503/cmaj.733267. CMAJ. 2017. PMID: 28827440 Free PMC article. No abstract available.
References
-
- Billings JA, Bernacki R. Strategic targeting of advance care planning interventions: the Goldilocks phenomenon. JAMA Intern Med 2014;174:620–4. - PubMed
-
- Spreeuwenberg C, Raats I, Teunissen S, et al. Development of a national care standard for palliative care in the Netherlands. Palliat Med 2014;28:634–5.
-
- Kersun L, Gyi L, Morrison WE. Training in difficult conversations: a national survey of pediatric hematology-oncology and pediatric critical care physicians. J Palliat Med 2009;12:525–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous