

Post Hoc Subanalysis of Two Randomized, Controlled Phase 3 Trials Evaluating Diclofenac Potassium for Oral Solution: Impact of Migraine-Associated Nausea and Prior Triptan Use on Efficacy
- PMID: 28386945
- PMCID: PMC5434944
- DOI: 10.1111/head.13073
Post Hoc Subanalysis of Two Randomized, Controlled Phase 3 Trials Evaluating Diclofenac Potassium for Oral Solution: Impact of Migraine-Associated Nausea and Prior Triptan Use on Efficacy
Abstract
Objective: To determine whether baseline nausea or prior triptan treatment for migraine impact the effectiveness of diclofenac potassium for oral solution in treating acute migraine.
Background: A great deal of variability exists in patients' response to migraine medications. Migraine-associated nausea is common and debilitating and can reduce the effectiveness of oral medications. It may cause patients to delay taking oral medications, which is known to diminish therapeutic outcomes, or to avoid taking them altogether. Gastroparesis, which may be associated with nausea, also inhibits drug absorption, resulting in lower bioavailability. Studies have shown that having nausea at the time of drug administration predicts a poorer response to triptan treatment. It is of interest to understand how effective other migraine medications are in patients with a poor response to triptans.
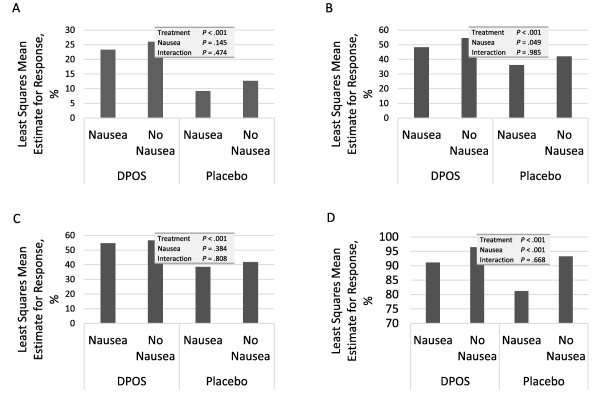
Methods: Data from two randomized, double-blind, placebo controlled trials were pooled and post hoc subgroup analyses were performed in patients with and without nausea at baseline, and in patients with and without prior triptan treatment. Efficacy assessments included the percentage of patients who, at 2 hours postdosing, were headache pain-free (2hPF, primary endpoint), without photophobia, without phonophobia, without nausea, or without a severe degree of disability. A Cochran-Mantel-Haenszel test, stratified by analysis center was used to evaluate treatment effect. Effects of nausea or prior triptan use were determined using logistic regression with factors of treatment group, analysis center, nausea or prior triptan use at time of dosing, and interaction of treatment group by nausea or prior triptan use at time of dosing.
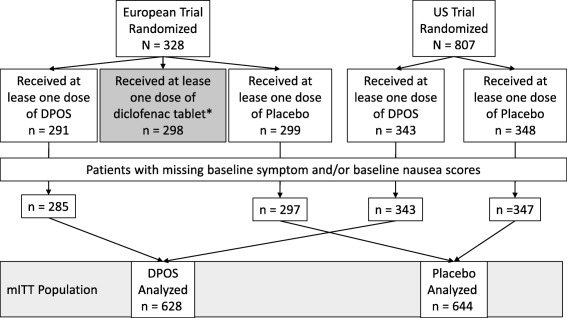
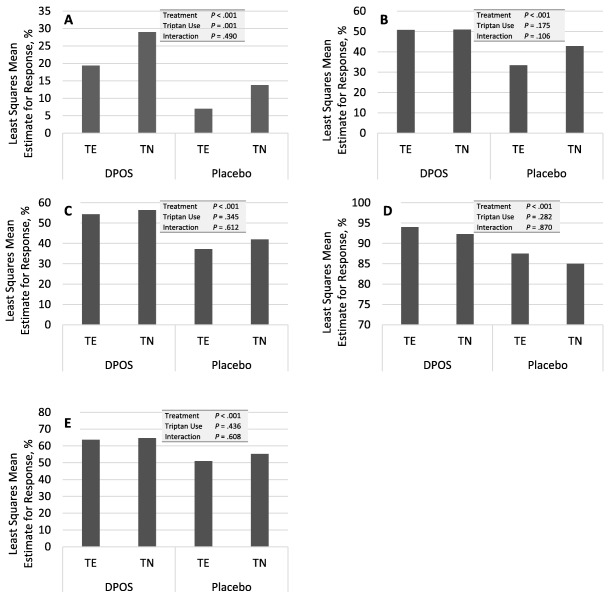
Results: The modified intent to treat population consisted of 1272 patients, 644 on active drug and 628 on placebo. The majority of patients (85%) were female. At the time of dosing, 783 (62%) patients reported nausea with the treated attack. Prior triptan use was recorded in 570 (45%). For headache pain, nausea, photophobia, and phonophobia, patients in the active treatment group had a statistically significantly better response than those receiving placebo, regardless of whether they had nausea at baseline. In logistic regression analysis only treatment group predicted a response for these parameters with no detectable group interaction. Baseline nausea, as well as treatment group, predicted whether patients recorded severe disability at 2 hours. While patients in the active treatment group were significantly more likely to be headache pain-free at 2 hours after dosing, whether or not they had previously been treated with triptan, more triptan-naïve patients (30%) than triptan-experienced patients (20%) were headache pain-free. Interestingly, in the placebo groups, triptan-naïve patients were also more likely to be PF (14% vs 7%). In the logistic regression analysis, treatment group predicted a headache pain response, triptan use predicted a lack of response, and there was no interaction between the two. Prior triptan use did not predict any of the other outcome measures.
Conclusions: Nausea at the time of dosing does not diminish the effectiveness of diclofenac potassium for oral solution. The rapid absorption profile may enhance the effectiveness in patients with nausea. Prior triptan use predicted poorer headache response at 2 hours postdose, suggesting the possibility of a subset of patients who are more likely to be refractory to both triptans and diclofenac. Diclofenac potassium for oral solution is effective in triptan-naïve patients but no reliable inference can be made from this study as to about how to order treatment.
Keywords: diclofenac potassium; migraine; nausea; oral solution; triptan; vomiting.
© 2017 The Authors Headache published by Wiley Periodicals, Inc. on behalf of American Headache Society.
Figures
Similar articles
-
Efficacy of ADAM Zolmitriptan for the Acute Treatment of Difficult-to-Treat Migraine Headaches.Headache. 2019 Apr;59(4):509-517. doi: 10.1111/head.13482. Epub 2019 Jan 30. Headache. 2019. PMID: 30698272 Free PMC article. Clinical Trial.
-
IM ketorolac vs diclofenac potassium powder for oral solution for the acute treatment of severe migraine: a randomized controlled trial.Neurol Sci. 2020 Mar;41(3):537-542. doi: 10.1007/s10072-019-04157-y. Epub 2019 Dec 12. Neurol Sci. 2020. PMID: 31833000 Clinical Trial.
-
Transdermal sumatriptan for acute treatment of migraineurs with baseline nausea.Headache. 2012 Feb;52(2):204-12. doi: 10.1111/j.1526-4610.2011.02065.x. Epub 2012 Jan 9. Headache. 2012. PMID: 22229837 Clinical Trial.
-
Pharmacological synergy: the next frontier on therapeutic advancement for migraine.Headache. 2012 Apr;52(4):636-47. doi: 10.1111/j.1526-4610.2011.02058.x. Epub 2012 Jan 6. Headache. 2012. PMID: 22221151 Review.
-
Diclofenac-potassium in migraine: a review.Drugs. 1999 Jun;57(6):991-1003. doi: 10.2165/00003495-199957060-00016. Drugs. 1999. PMID: 10400409 Review.
Cited by
-
Pathophysiology and Therapy of Associated Features of Migraine.Cells. 2022 Sep 5;11(17):2767. doi: 10.3390/cells11172767. Cells. 2022. PMID: 36078174 Free PMC article. Review.
-
Efficacy of ubrogepant based on prior exposure and response to triptans: A post hoc analysis.Headache. 2021 Mar;61(3):422-429. doi: 10.1111/head.14089. Epub 2021 Mar 22. Headache. 2021. PMID: 33749826 Free PMC article. Clinical Trial.
References
-
- Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: Updated statistics from government health surveillance studies. Headache. 2015;55:21‐34. - PubMed
-
- Becker WJ. Acute migraine treatment in adults. Headache. 2015;55:778‐793. - PubMed
-
- Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: The American Headache Society evidence assessment of migraine pharmacotherapies. Headache. 2015;55:3‐20. - PubMed
-
- Bigal M, Rapoport A, Aurora S, Sheftell F, Tepper S, Dahlof C. Satisfaction with current migraine therapy: Experience from 3 centers in US and Sweden. Headache. 2007;47:475‐479. - PubMed
-
- Katic BJ, Rajagopalan S, Ho TW, Chen YT, Hu XH. Triptan persistency among newly initiated users in a pharmacy claims database. Cephalalgia. 2011;31:488‐500. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
