

Review
. 2017 Apr;5(2):10.1128/microbiolspec.tnmi7-0037-2016.
doi: 10.1128/microbiolspec.TNMI7-0037-2016.
Tuberculosis in Infants and Children
Affiliations
- PMID: 28387193
- PMCID: PMC11687478
- DOI: 10.1128/microbiolspec.TNMI7-0037-2016
Item in Clipboard
Review
Tuberculosis in Infants and Children
Microbiol Spectr.
2017 Apr.
Abstract
One million children develop tuberculosis disease each year, and 210,000 die from complications of tuberculosis. Childhood tuberculosis is very different from adult tuberculosis in epidemiology, clinical and radiographic presentation, and treatment. This review highlights the many unique features of childhood tuberculosis, with special emphasis on very young children and adolescents, who are most likely to develop disease after infection has occurred.
Figures
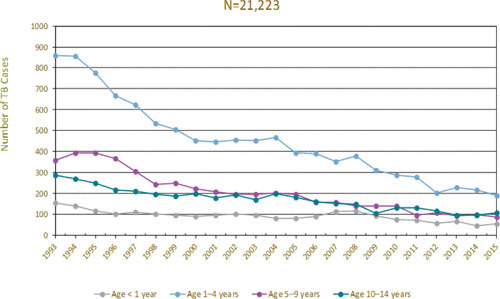
Tuberculosis (TB) case rates by age group for children, 1993 to 2015. (Data in the public domain, courtesy of the CDC.)
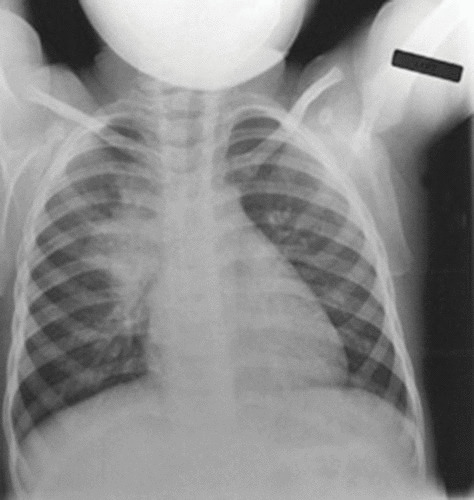
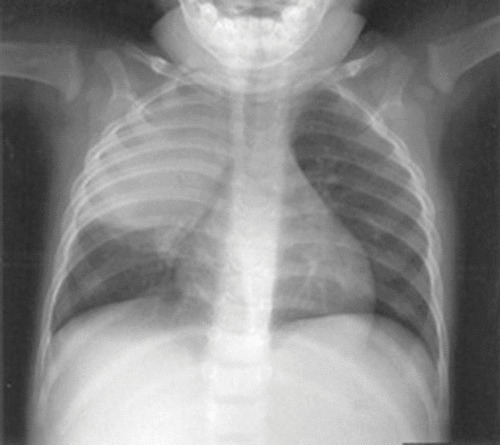
Early collapse-consolidation lesion in a child with tuberculosis. Mediastinal adenopathy also is present on the right side.
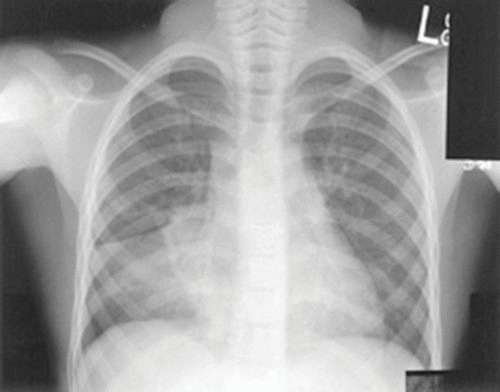
Slightly more extensive right-sided adenopathy with atelectasis in a 2-year-old with tuberculosis.
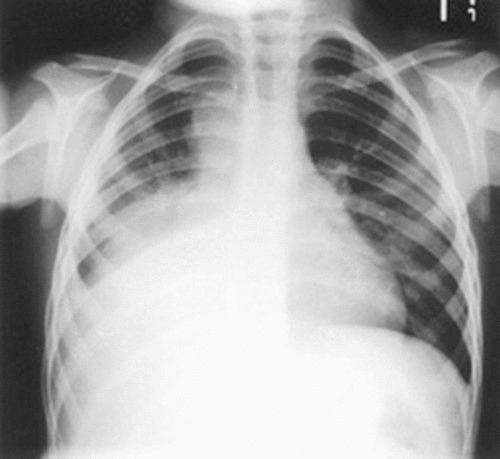
Well-formed collapse-consolidation lesion on the right, with large mediastinal and hilar adenopathy and atelectasis.
Tuberculous pneumonia with bowing of the horizontal fissure. Children with this finding may have an associated bacterial infection.
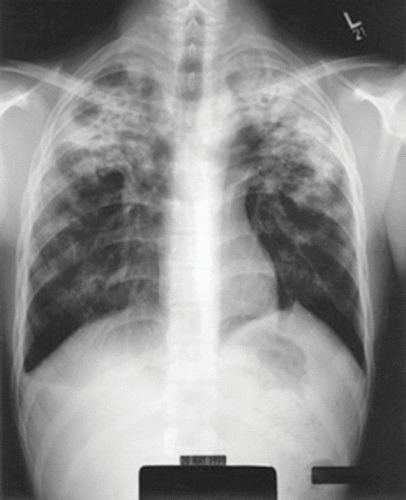
Reactivation-type tuberculosis in an adolescent boy.
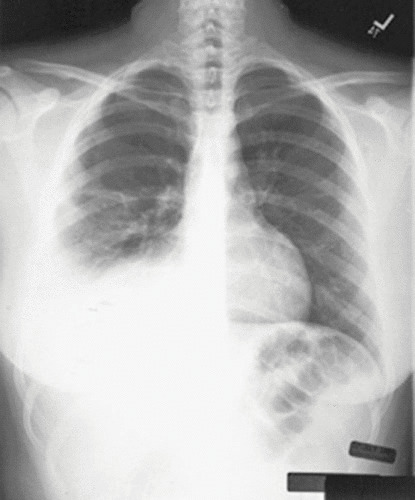
A tuberculous pleural effusion in an adolescent girl.
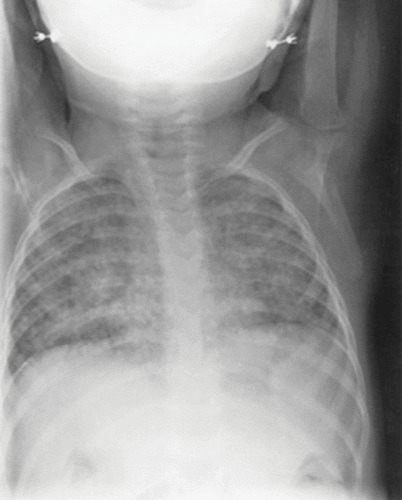
Miliary tuberculosis in an infant. The child presented with fever and respiratory distress.
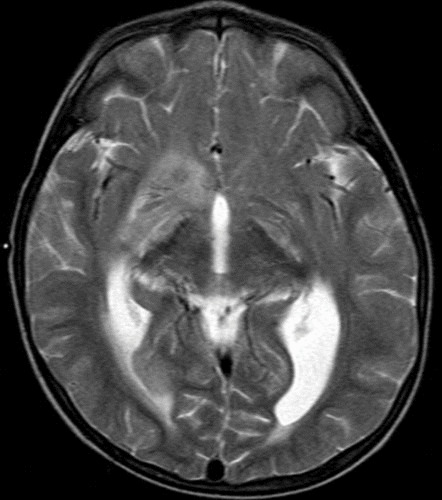
Magnetic resonance imaging showing abnormal enhancement along the basilar cisterns, acute ischemia or possibly cerebritis involving the right caudate head, right putaminal and possibly right globus pallidus, ventriculomegaly (ventriculoperitoneal shunt in place), and enhancement along multiple cranial nerves.
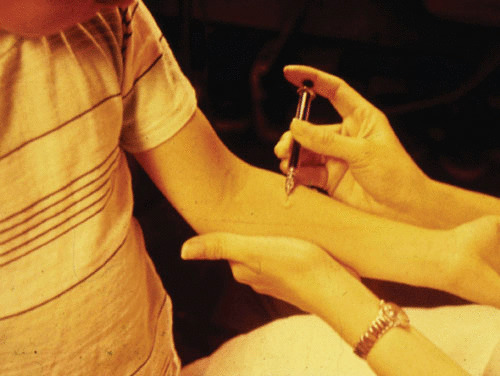
A helpful technique for applying the Mantoux TST on a child. The hand is anchored on the side of the child’s arm, providing stability. The tuberculin is injected in a lateral direction.
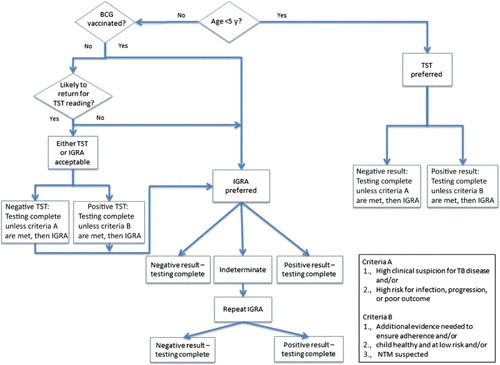
An algorithm for the use of the TST and IGRAs in children. Entry into the algorithm assumes that the child has at least 1 risk factor for TB infection. Note: many experts use age <2 years as the starting point. Reprinted from reference , with permission from the American Academy of Pediatrics Committee on Infectious Diseases.
Similar articles
-
Reducing tuberculosis incidence in HIV-infected patients by tuberculin skin testing, preventive treatment, and antiretroviral therapy.Clin Infect Dis. 2007 May 15;44(10):1393-4; author reply 1394-5. doi: 10.1086/516608. Clin Infect Dis. 2007. PMID: 17443486 No abstract available.
-
Impact of human immunodeficiency virus 1 infection on clinical presentation, treatment outcome and survival in a cohort of Ethiopian children with tuberculosis.Pediatr Infect Dis J. 2002 Nov;21(11):1053-61. doi: 10.1097/00006454-200211000-00016. Pediatr Infect Dis J. 2002. PMID: 12442029 Clinical Trial.
-
[Methods of detection and characteristics of clinical manifestations of tuberculosis in children and adolescents].Probl Tuberk. 1995;(5):22-4. Probl Tuberk. 1995. PMID: 7567884 Russian.
-
Tuberculosis in infants, children, and adolescents: an update with case studies.Pediatr Nurs. 1998 Sep-Oct;24(5):411-6, 419-20. Pediatr Nurs. 1998. PMID: 9832901 Review.
-
BCG vaccination in India and tuberculosis in children: newer facets.Indian J Pediatr. 1994 Sep-Oct;61(5):451-62. doi: 10.1007/BF02751703. Indian J Pediatr. 1994. PMID: 7744445 Review.
Cited by
-
Efficacy and safety of CO2 cryotherapy in the treatment of infants with tracheobronchial tuberculosis.Front Pediatr. 2022 Oct 10;10:984738. doi: 10.3389/fped.2022.984738. eCollection 2022. Front Pediatr. 2022. PMID: 36299689 Free PMC article.
-
Prognostic Model for Progradient Tuberculosis Course in HIV-Infected Children.Sovrem Tekhnologii Med. 2020;12(2):74-78. doi: 10.17691/stm2020.12.2.09. Sovrem Tekhnologii Med. 2020. PMID: 34513056 Free PMC article.
-
Research of childhood tuberculosis in suspected populations by molecular methods: A multicenter study in China.Front Cell Infect Microbiol. 2022 Oct 19;12:1018699. doi: 10.3389/fcimb.2022.1018699. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36339333 Free PMC article.
-
A Mitocentric View of the Main Bacterial and Parasitic Infectious Diseases in the Pediatric Population.Int J Mol Sci. 2021 Mar 23;22(6):3272. doi: 10.3390/ijms22063272. Int J Mol Sci. 2021. PMID: 33806981 Free PMC article. Review.
-
Evaluation of Xpert MTB/RIF Ultra Assay for Diagnosis of Childhood Tuberculosis: a Multicenter Accuracy Study.J Clin Microbiol. 2020 Aug 24;58(9):e00702-20. doi: 10.1128/JCM.00702-20. Print 2020 Aug 24. J Clin Microbiol. 2020. PMID: 32522831 Free PMC article.
References
-
- Jaganath D, Zalwango S, Okware B, Nsereko M, Kisingo H, Malone L, Lancioni C, Okwera A, Joloba M, Mayanja-Kizza H, Boom WH, Stein C, Mupere E, Tuberculosis Research Unit. 2013. Contact investigation for active tuberculosis among child contacts in Uganda. Clin Infect Dis 57:1685–1692. [PubMed] - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
