

Analysis of free text in electronic health records for identification of cancer patient trajectories
- PMID: 28387314
- PMCID: PMC5384191
- DOI: 10.1038/srep46226
Analysis of free text in electronic health records for identification of cancer patient trajectories
Abstract
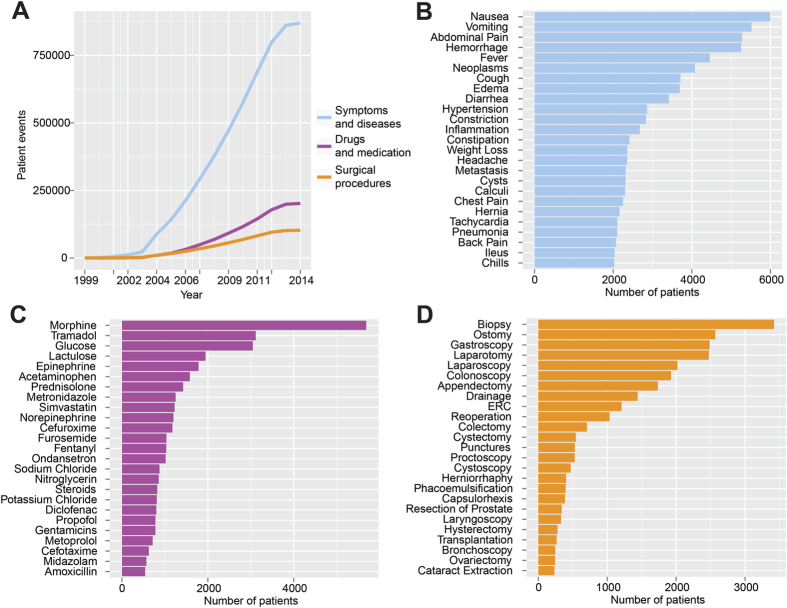
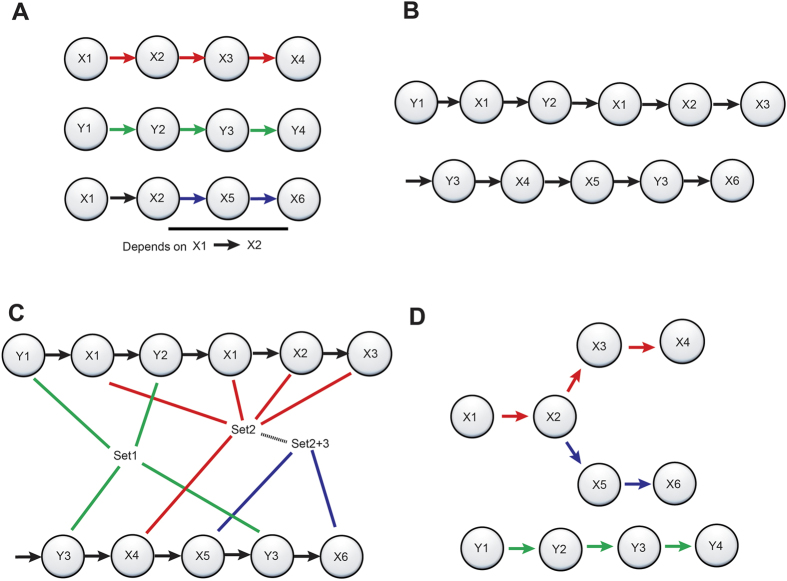
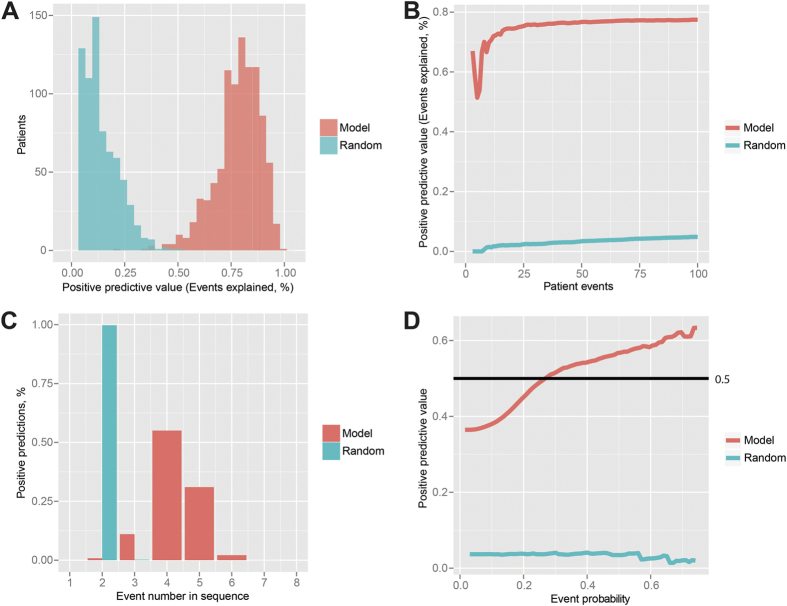
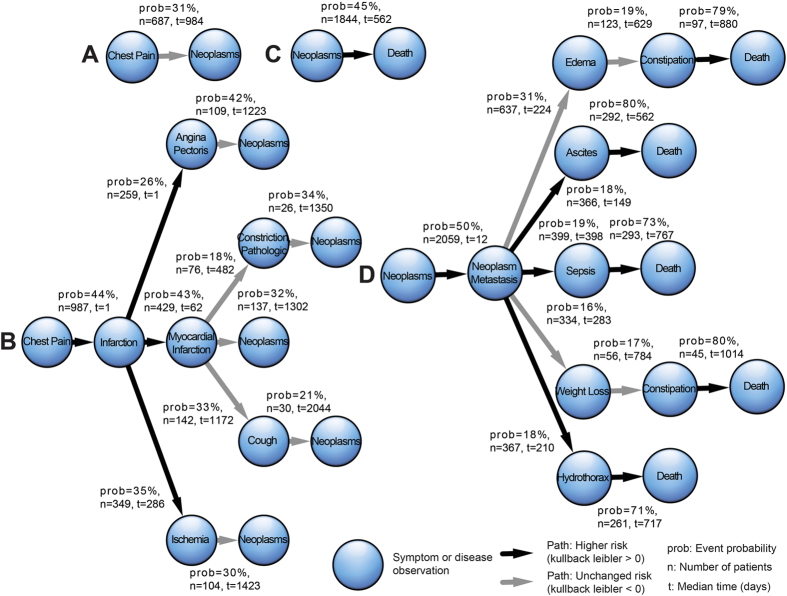
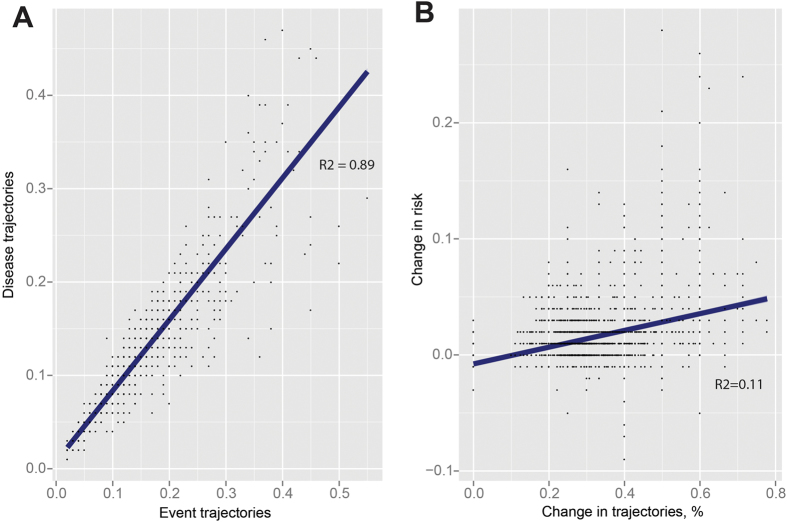
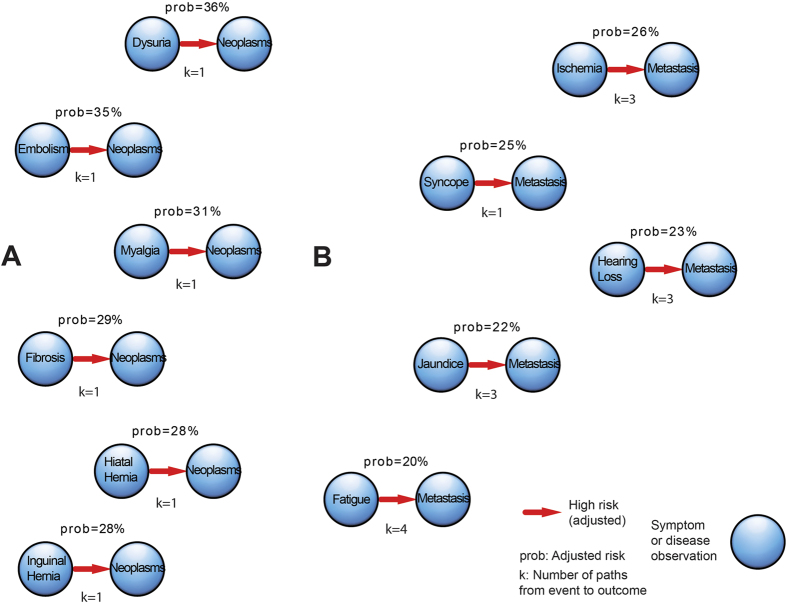
With an aging patient population and increasing complexity in patient disease trajectories, physicians are often met with complex patient histories from which clinical decisions must be made. Due to the increasing rate of adverse events and hospitals facing financial penalties for readmission, there has never been a greater need to enforce evidence-led medical decision-making using available health care data. In the present work, we studied a cohort of 7,741 patients, of whom 4,080 were diagnosed with cancer, surgically treated at a University Hospital in the years 2004-2012. We have developed a methodology that allows disease trajectories of the cancer patients to be estimated from free text in electronic health records (EHRs). By using these disease trajectories, we predict 80% of patient events ahead in time. By control of confounders from 8326 quantified events, we identified 557 events that constitute high subsequent risks (risk > 20%), including six events for cancer and seven events for metastasis. We believe that the presented methodology and findings could be used to improve clinical decision support and personalize trajectories, thereby decreasing adverse events and optimizing cancer treatment.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Frankovich J., Longhurst C. A. & Sutherland S. M. Evidence-Based Medicine in the EMR Era. N. Engl. J. Med. 365, 1758–1759 (2011). - PubMed
-
- Sell S. Readmissions within 30 days cost the NHS £1.6bn a year. GP-Online Available at: http://www.gponline.com/readmissions-within-30-days-cost-nhs-16bn-year/a... (2010).
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
