

Near-infrared fluorescent image-guided surgery for intracranial meningioma
- PMID: 28387632
- PMCID: PMC10985532
- DOI: 10.3171/2016.10.JNS161636
Near-infrared fluorescent image-guided surgery for intracranial meningioma
Abstract
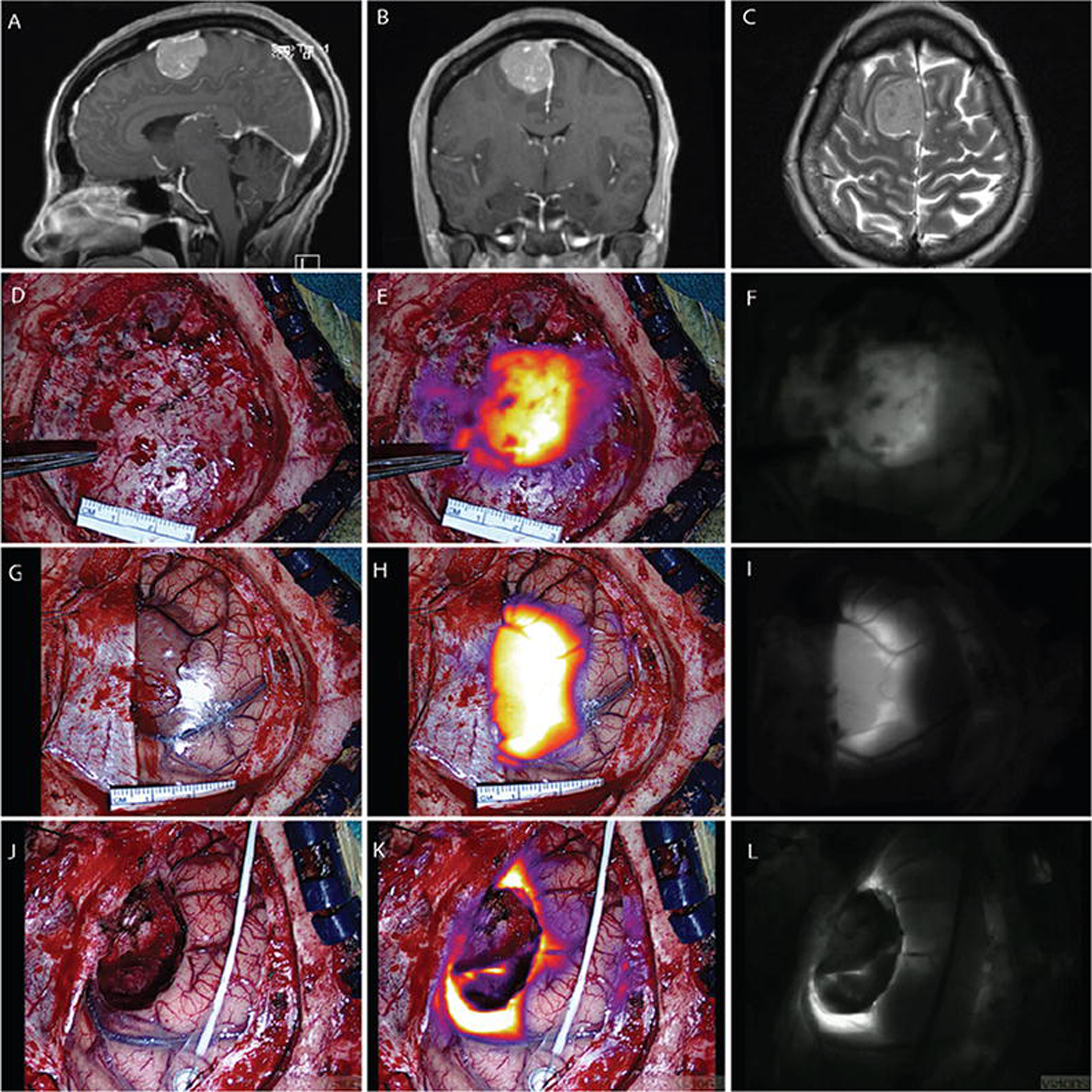
OBJECTIVE Meningiomas are the most common primary tumor of the central nervous system. Complete resection can be curative, but intraoperative identification of dural tails and tumor remnants poses a clinical challenge. Given data from preclinical studies and previous clinical trials, the authors propose a novel method of localizing tumor tissue and identifying residual disease at the margins via preoperative systemic injection of a near-infrared (NIR) fluorescent contrast dye. This technique, what the authors call "second-window indocyanine green" (ICG), relies on the visualization of ICG approximately 24 hours after intravenous injection. METHODS Eighteen patients were prospectively identified and received 5 mg/kg of second-window ICG the day prior to surgery. An NIR camera was used to localize the tumor prior to resection and to inspect the margins following standard resection. The signal to background ratio (SBR) of the tumor to the normal brain parenchyma was measured in triplicate. Gross tumor and margin specimens were qualitatively reported with respect to fluorescence. Neuropathological diagnosis served as the reference gold standard to calculate the sensitivity and specificity of the imaging technique. RESULTS Eighteen patients harbored 15 WHO Grade I and 3 WHO Grade II meningiomas. Near-infrared visualization during surgery ranged from 18 to 28 hours (mean 23 hours) following second-window ICG infusion. Fourteen of the 18 tumors demonstrated a markedly elevated SBR of 5.6 ± 1.7 as compared with adjacent brain parenchyma. Four of the 18 patients showed an inverse pattern of NIR signal, that is, stronger in the adjacent normal brain than in the tumor (SBR 0.31 ± 0.1). The best predictor of inversion was time from injection, as the patients who were imaged earlier were more likely to demonstrate an appropriate SBR. The second-window ICG technique demonstrated a sensitivity of 96.4%, specificity of 38.9%, positive predictive value of 71.1%, and a negative predictive value of 87.5% for tumor. CONCLUSIONS Systemic injection of NIR second-window ICG the day before surgery can be used to visualize meningiomas intraoperatively. Intraoperative NIR imaging provides higher sensitivity in identifying meningiomas than the unassisted eye. In this study, 14 of the 18 patients with meningioma demonstrated a strong SBR compared with adjacent brain. In the future, reducing the time interval from dye injection to intraoperative imaging may improve fluorescence at the margins, though this approach requires further investigation. Clinical trial registration no.: NCT02280954 ( clincialtrials.gov ).
Keywords: 125IR; 5-ALA = 5-aminolevulinic acid; EPR = enhanced permeability and retention; ICG = indocyanine green; NIR = near-infrared dye; NPV = negative predictive value; PPV = positive predictive value; ROC = receiver operating characteristic; SBR = signal to background ratio; brain tumor; fluorescence; indocyanine green; meningioma; near infrared; oncology.
Figures



References
-
- Alacam B, Yazici B, Intes X, Chance B: Analysis of ICG pharmacokinetics in cancerous tumors using NIR optical methods. Conf Proc IEEE Eng Med Biol Soc 1:62–65, 2005 - PubMed
-
- Borovich B, Doron Y: Recurrence of intracranial meningiomas: the role played by regional multicentricity. J Neurosurg 64:58–63, 1986 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
