

Association between diabetic foot ulcer and diabetic retinopathy
- PMID: 28388680
- PMCID: PMC5384753
- DOI: 10.1371/journal.pone.0175270
Association between diabetic foot ulcer and diabetic retinopathy
Abstract
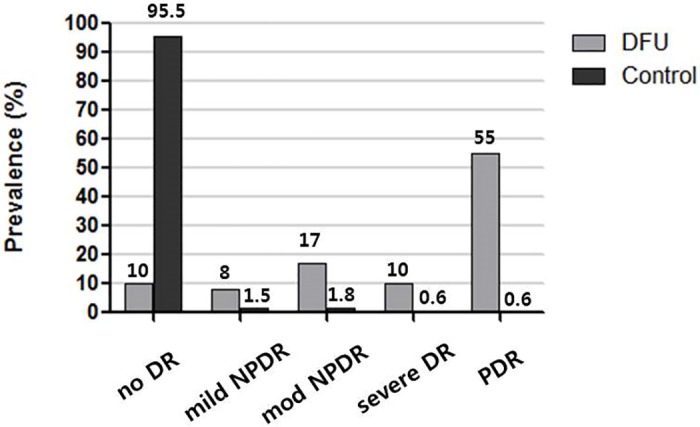
Purpose: We aimed to investigate the prevalence of diabetic retinopathy (DR) in patients with diabetic foot ulcer (DFU) and elucidate the association between DR and DFU severities and their shared risk factors.
Methods: A retrospective review was conducted on DFU patients who underwent ophthalmic and vascular examinations within 6 months; 100 type 2 diabetic patients with DFU were included. The medical records of 2496 type 2 diabetic patients without DFU served as control data. DR prevalence and severity were assessed in DFU patients. DFU patients were compared with the control group regarding each clinical variable. Additionally, DFU patients were divided into two groups according to DR severity and compared.
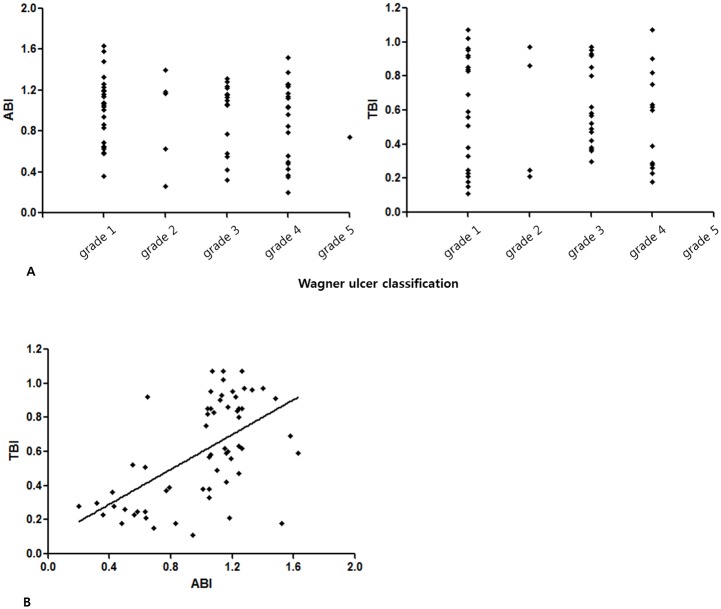
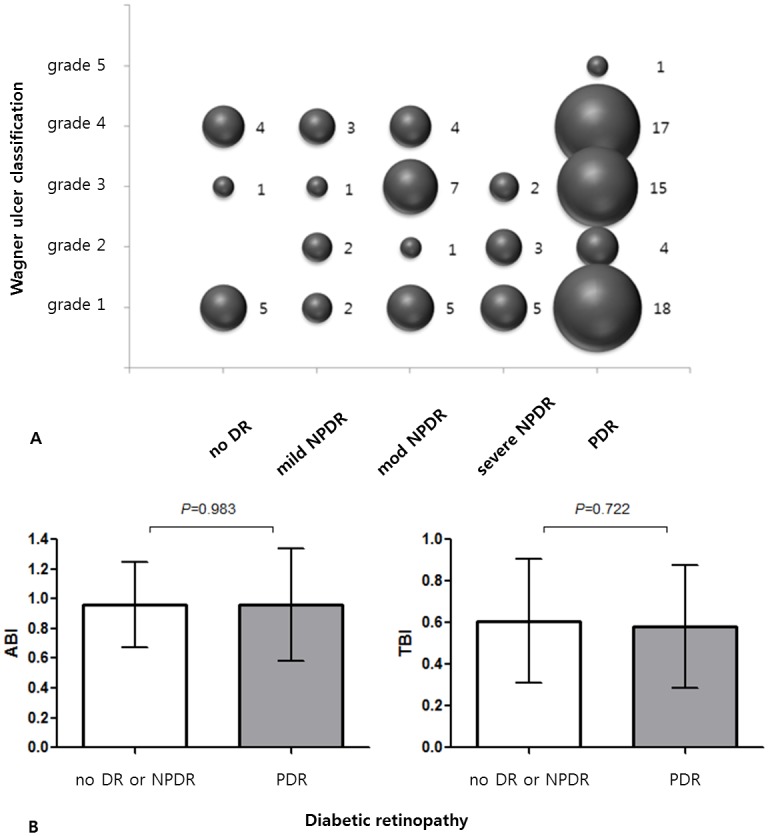
Results: Out of 100 DFU patients, 90 patients (90%) had DR and 55 (55%) had proliferative DR (PDR). There was no significant association between DR and DFU severities (R = 0.034, p = 0.734). A multivariable analysis comparing type 2 diabetic patients with and without DFUs showed that the presence of DR [OR, 226.12; 95% confidence interval (CI), 58.07-880.49; p < 0.001] and proliferative DR [OR, 306.27; 95% CI, 64.35-1457.80; p < 0.001), higher HbA1c (%, OR, 1.97, 95% CI, 1.46-2.67; p < 0.001), higher serum creatinine (mg/dL, OR, 1.62, 95% CI, 1.06-2.50; p = 0.027), older age (years, OR, 1.12; 95% CI, 1.06-1.17; p < 0.001), higher pulse pressure (mmHg, OR, 1.03; 95% CI, 1.00-1.06; p = 0.025), lower cholesterol (mg/dL, OR, 0.94; 95% CI, 0.92-0.97; p < 0.001), lower BMI (kg/m2, OR, 0.87, 95% CI, 0.75-1.00; p = 0.044) and lower hematocrit (%, OR, 0.80, 95% CI, 0.74-0.87; p < 0.001) were associated with DFUs. In a subgroup analysis of DFU patients, the PDR group had a longer duration of diabetes mellitus, higher serum BUN, and higher serum creatinine than the non-PDR group. In the multivariable analysis, only higher serum creatinine was associated with PDR in DFU patients (OR, 1.37; 95% CI, 1.05-1.78; p = 0.021).
Conclusions: Diabetic retinopathy is prevalent in patients with DFU and about half of DFU patients had PDR. No significant association was found in terms of the severity of these two diabetic complications. To prevent blindness, patients with DFU, and especially those with high serum creatinine, should undergo retinal examinations for timely PDR diagnosis and management.
Conflict of interest statement
Figures
Similar articles
-
[Diabetes self-management and its association with diabetic retinopathy in patients with type 2 diabetes].Zhonghua Yan Ke Za Zhi. 2013 Jun;49(6):500-6. Zhonghua Yan Ke Za Zhi. 2013. PMID: 24119962 Chinese.
-
Diabetic Retinopathy in Patients With Diabetic Foot Ulcer: A Systematic Review.Int J Low Extrem Wounds. 2021 Jun;20(2):98-103. doi: 10.1177/1534734620982237. Epub 2020 Dec 22. Int J Low Extrem Wounds. 2021. PMID: 33353439
-
Thailand diabetes registry project: prevalence of diabetic retinopathy and associated factors in type 1 diabetes mellitus.J Med Assoc Thai. 2006 Aug;89 Suppl 1:S17-26. J Med Assoc Thai. 2006. PMID: 17715830
-
An assessment of peripheral vascular disease in patients with diabetic foot ulcer.Foot (Edinb). 2010 Dec;20(4):114-7. doi: 10.1016/j.foot.2010.09.002. Epub 2010 Oct 15. Foot (Edinb). 2010. PMID: 20951569
-
Uric Acid and Diabetic Retinopathy: A Systematic Review and Meta-Analysis.Front Public Health. 2022 May 31;10:906760. doi: 10.3389/fpubh.2022.906760. eCollection 2022. Front Public Health. 2022. PMID: 35712295 Free PMC article.
Cited by
-
Exploring Different Strategies of Assessing the Economic Impact of Multiple Diabetes-Associated Complications and Their Interactions: A Large Claims-Based Study in Germany.Pharmacoeconomics. 2019 Jan;37(1):63-74. doi: 10.1007/s40273-018-0699-1. Pharmacoeconomics. 2019. PMID: 30167918
-
Protective effect of high mobility group box-1 silence on diabetic retinopathy: an in vivo study.Int J Clin Exp Pathol. 2017 Aug 1;10(8):8148-8160. eCollection 2017. Int J Clin Exp Pathol. 2017. PMID: 31966667 Free PMC article.
-
Diabetic retinopathy in patients with diabetic foot syndrome in South India.Indian J Ophthalmol. 2018 Apr;66(4):547-550. doi: 10.4103/ijo.IJO_1000_17. Indian J Ophthalmol. 2018. PMID: 29582817 Free PMC article.
-
Incidence of Diabetic Foot Ulcer and Its Predictors Among Diabetes Mellitus Patients at Felege Hiwot Referral Hospital, Bahir Dar, Northwest Ethiopia: A Retrospective Follow-Up Study.Diabetes Metab Syndr Obes. 2020 Oct 14;13:3703-3711. doi: 10.2147/DMSO.S280152. eCollection 2020. Diabetes Metab Syndr Obes. 2020. PMID: 33116720 Free PMC article.
-
Differentiation of Diabetic Foot Ulcers Based on Stimulation of Myogenic Oscillations by Transient Ischemia.Vasc Health Risk Manag. 2021 Apr 19;17:145-152. doi: 10.2147/VHRM.S307366. eCollection 2021. Vasc Health Risk Manag. 2021. PMID: 33907408 Free PMC article.
References
-
- Apelqvist J, Larsson J. What is the most effective way to reduce incidence of amputation in the diabetic foot? Diabetes Metab Res Rev. 2000;16 Suppl 1:S75–83. - PubMed
-
- Prompers L, Schaper N, Apelqvist J, Edmonds M, Jude E, Mauricio D, et al. Prediction of outcome in individuals with diabetic foot ulcers: focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia. 2008;51(5):747–55. 10.1007/s00125-008-0940-0 - DOI - PMC - PubMed
-
- Moss SE, Klein R, Klein BE. The prevalence and incidence of lower extremity amputation in a diabetic population. Arch Intern Med. 1992;152(3):610–6. - PubMed
-
- Borssen B, Bergenheim T, Lithner F. The epidemiology of foot lesions in diabetic patients aged 15–50 years. Diabet Med. 1990;7(5):438–44. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
