

What are the risks and benefits of temporarily discontinuing medications to prevent acute kidney injury? A systematic review and meta-analysis
- PMID: 28389482
- PMCID: PMC5541442
- DOI: 10.1136/bmjopen-2016-012674
What are the risks and benefits of temporarily discontinuing medications to prevent acute kidney injury? A systematic review and meta-analysis
Abstract
Objectives: To summarise evidence on temporary discontinuation of medications to prevent acute kidney injury (AKI).
Design: Systematic review and meta-analysis of randomised and non-randomised studies.
Participants: Adults taking diuretics, ACE inhibitors (ACEI), angiotensin receptor blockers (ARB), direct renin inhibitors, non-steroidal anti-inflammatories, metformin or sulfonylureas, experiencing intercurrent illnesses, radiological or surgical procedures.
Interventions: Temporary discontinuation of any of the medications of interest.
Primary and secondary outcome measures: Risk of AKI. Secondary outcome measures were estimated glomerular filtration rate and creatinine post-AKI, urea, systolic and diastolic blood pressure, death, clinical outcomes and biomarkers.
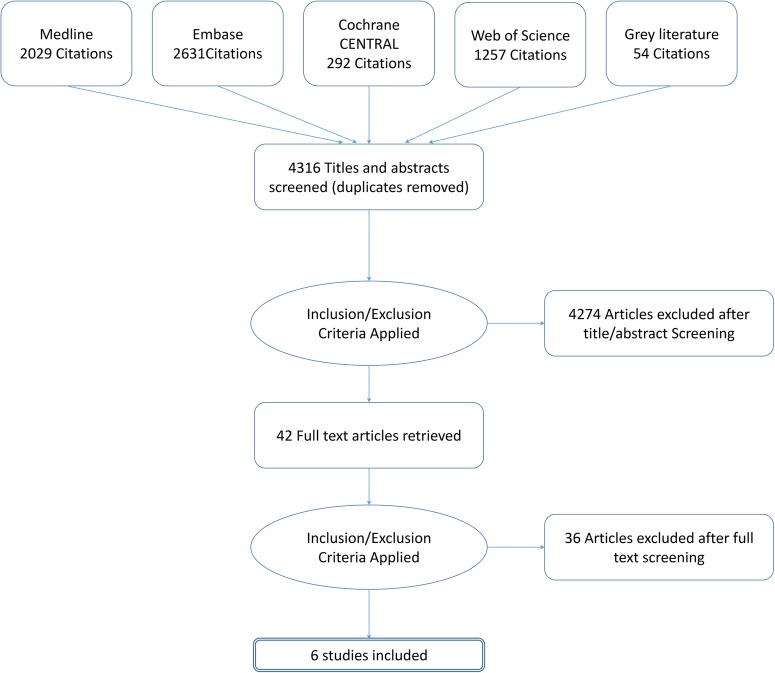
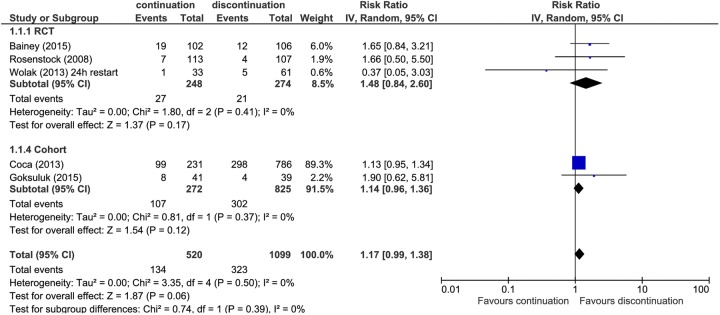
Results: 6 studies were included (1663 participants), 3 randomised controlled trials (RCTs) and 3 prospective cohort studies. The mean age ranged from 65 to 73 years, and the proportion of women ranged from 31% to 52%. All studies were in hospital settings; 5 evaluated discontinuation of medication prior to coronary angiography and 1 prior to cardiac surgery. 5 studies evaluated discontinuation of ACEI and ARBs and 1 small cohort study looked at discontinuation of non-steroidal anti-inflammatory drugs. No studies evaluated discontinuation of medication in the community following an acute intercurrent illness. There was an increased risk of AKI of around 15% in those in whom medication was continued compared with those in whom it was discontinued (relative risk (RR) 1.17, 95% CI 0.99 to 1.38; 5 studies). When only results from RCTs were pooled, the increase in risk was almost 50% (RR 1.48, 95% CI 0.84 to 2.60; 3 RCTs), but the CI was wider. There was no difference between groups for any secondary outcomes.
Conclusions: There is low-quality evidence that withdrawal of ACEI/ARBs prior to coronary angiography and cardiac surgery may reduce the incidence of AKI. There is no evidence of the impact of drug cessation interventions on AKI incidence during intercurrent illness in primary or secondary care.
Trial registration number: PROSPERO CRD42015023210.
Keywords: Acute kidney injury; Angiotensin receptor blockers; Angiotensin-converting enzyme inhibitors; Medication discontinuation; NSAIDs; Sick day rules.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures


References
-
- National Confidential Enquiry into Patient Outcome and Death. Acute Kidney Injury: Adding Insult to Injury. 2009. http://www.ncepod.org.uk/2009aki.html
-
- Think Kidneys. Acute Kidney Injury: the NHS campaign to improve the care of people at risk of, or with, acute kidney injury. 2016. (11 April 2016). https://www.thinkkidneys.nhs.uk/aki/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous