

Prognostic Value of Noninvasive Cardiovascular Testing in Patients With Stable Chest Pain: Insights From the PROMISE Trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain)
- PMID: 28389572
- PMCID: PMC5946057
- DOI: 10.1161/CIRCULATIONAHA.116.024360
Prognostic Value of Noninvasive Cardiovascular Testing in Patients With Stable Chest Pain: Insights From the PROMISE Trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain)
Abstract
Background: Optimal management of patients with stable chest pain relies on the prognostic information provided by noninvasive cardiovascular testing, but there are limited data from randomized trials comparing anatomic with functional testing.
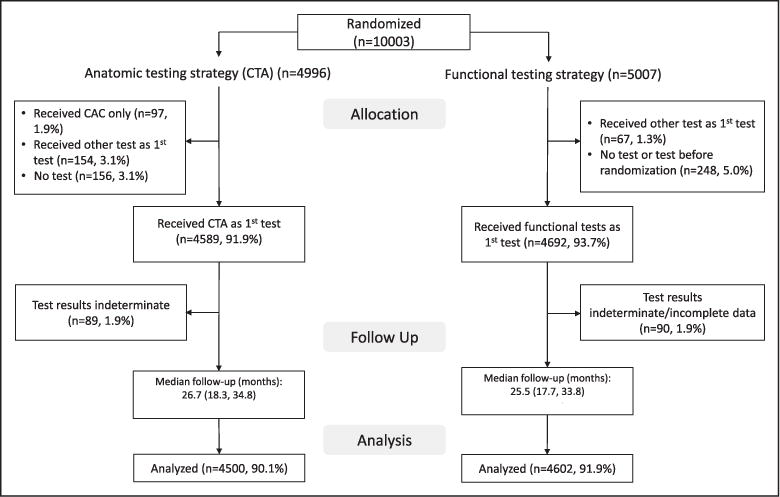
Methods: In the PROMISE trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain), patients with stable chest pain and intermediate pretest probability for obstructive coronary artery disease (CAD) were randomly assigned to functional testing (exercise electrocardiography, nuclear stress, or stress echocardiography) or coronary computed tomography angiography (CTA). Site-based diagnostic test reports were classified as normal or mildly, moderately, or severely abnormal. The primary end point was death, myocardial infarction, or unstable angina hospitalizations over a median follow-up of 26.1 months.
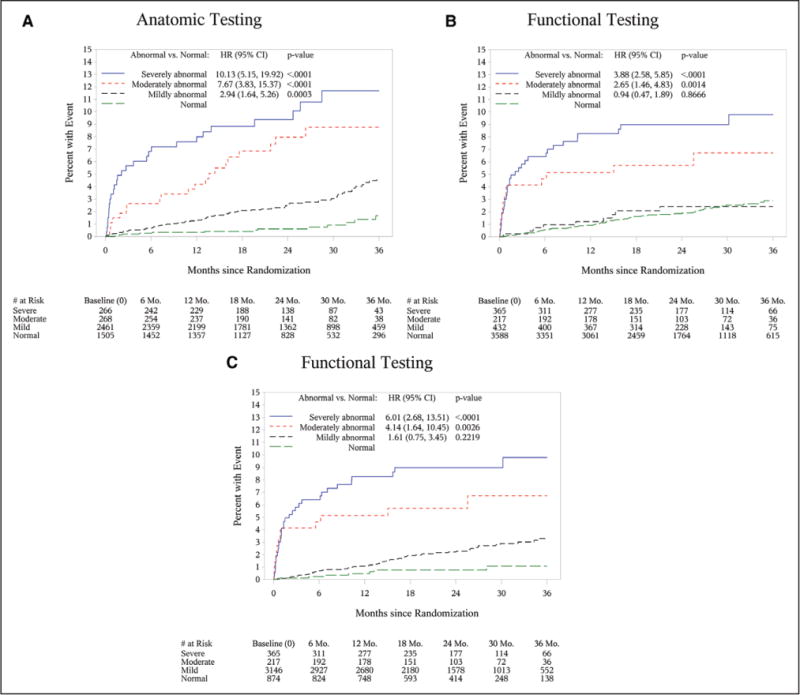
Results: Both the prevalence of normal test results and incidence rate of events in these patients were significantly lower among 4500 patients randomly assigned to CTA in comparison with 4602 patients randomly assigned to functional testing (33.4% versus 78.0%, and 0.9% versus 2.1%, respectively; both P<0.001). In CTA, 54.0% of events (n=74/137) occurred in patients with nonobstructive CAD (1%-69% stenosis). Prevalence of obstructive CAD and myocardial ischemia was low (11.9% versus 12.7%, respectively), with both findings having similar prognostic value (hazard ratio, 3.74; 95% confidence interval [CI], 2.60-5.39; and 3.47; 95% CI, 2.42-4.99). When test findings were stratified as mildly, moderately, or severely abnormal, hazard ratios for events in comparison with normal tests increased proportionally for CTA (2.94, 7.67, 10.13; all P<0.001) but not for corresponding functional testing categories (0.94 [P=0.87], 2.65 [P=0.001], 3.88 [P<0.001]). The discriminatory ability of CTA in predicting events was significantly better than functional testing (c-index, 0.72; 95% CI, 0.68-0.76 versus 0.64; 95% CI, 0.59-0.69; P=0.04). If 2714 patients with at least an intermediate Framingham Risk Score (>10%) who had a normal functional test were reclassified as being mildly abnormal, the discriminatory capacity improved to 0.69 (95% CI, 0.64-0.74).
Conclusions: Coronary CTA, by identifying patients at risk because of nonobstructive CAD, provides better prognostic information than functional testing in contemporary patients who have stable chest pain with a low burden of obstructive CAD, myocardial ischemia, and events.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01174550.
Keywords: coronary artery disease; diagnostic tests, routine; prognosis.
© 2017 American Heart Association, Inc.
Conflict of interest statement
The other authors report no potential conflicts of interest.
Figures
Comment in
-
New Promises for Refining Risk Stratification From Anatomical and Functional Assessment of Stable Chest Pain.Circulation. 2017 Jun 13;135(24):2333-2335. doi: 10.1161/CIRCULATIONAHA.117.028637. Circulation. 2017. PMID: 28606947 No abstract available.
-
Letter by Jin-shan and Xue-bin Regarding Article, "Prognostic Value of Noninvasive Cardiovascular Testing in Patients With Stable Chest Pain: Insights From the PROMISE Trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain)".Circulation. 2017 Nov 28;136(22):2202-2203. doi: 10.1161/CIRCULATIONAHA.117.030674. Circulation. 2017. PMID: 29180500 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB, American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–322. doi: 10.1161/CIR.0000000000000152. - DOI - PubMed
-
- SCOT-HEART Investigators. CT Coronary Angiography in Patients With Suspected Angina Due to Coronary Heart Disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385:2383–2391. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
