

Modeling therapeutic response to radioiodine in metastatic thyroid cancer: a proof-of-concept study for individualized medicine
- PMID: 28389624
- PMCID: PMC5503603
- DOI: 10.18632/oncotarget.16637
Modeling therapeutic response to radioiodine in metastatic thyroid cancer: a proof-of-concept study for individualized medicine
Abstract
Purpose: Radioiodine therapy (RAI) has traditionally been used as treatment for metastatic thyroid cancer, based on its ability to concentrate iodine. Propositions to maximize tumor response with minimizing toxicity, must recognize the infinite possibilities of empirical tests. Therefore, an approach of this study was to build a mathematical model describing tumor growth with the kinetics of thyroglobulin (Tg) concentrations over time, following RAI for metastatic thyroid cancer.
Experimental design: Data from 50 patients with metastatic papillary thyroid carcinoma treated within eight French institutions, followed over 3 years after initial RAI treatments, were included in the model. A semi-mechanistic mathematical model that describes the tumor growth under RAI treatment was designed.
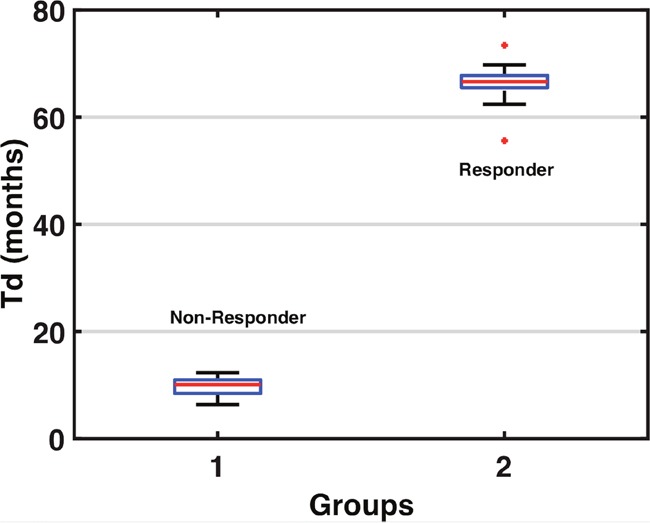
Results: Our model was able to separate patients who responded to RAI from those who did not, concordant with the physicians' determination of therapeutic response. The estimated tumor doubling-time (Td was found to be the most informative parameter for the distinction between responders and non-responders. The model was also able to reclassify particular patients in early treatment stages.
Conclusions: The results of the model present classification criteria that could indicate whether patients will respond or not to RAI treatment, and provide the opportunity to perform personalized management plans.
Keywords: mathematical model; metastatic thyroid cancer; personalized medicine; radioactive iodine therapy; therapeutic nuclear medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Clinical outcome of patients with papillary thyroid carcinoma who have recurrence after initial radioactive iodine therapy.Cancer. 1996 Aug 1;78(3):493-501. doi: 10.1002/(SICI)1097-0142(19960801)78:3<493::AID-CNCR17>3.0.CO;2-U. Cancer. 1996. PMID: 8697396
-
Clinical outcomes following empiric radioiodine therapy in patients with structurally identifiable metastatic follicular cell-derived thyroid carcinoma with negative diagnostic but positive post-therapy 131I whole-body scans.Thyroid. 2012 Sep;22(9):877-83. doi: 10.1089/thy.2011.0429. Epub 2012 Jul 24. Thyroid. 2012. PMID: 22827641
-
Pulmonary metastases in children and adolescents with papillary thyroid cancer in China: prognostic factors and outcomes from treatment with 131I.Endocrine. 2018 Oct;62(1):149-158. doi: 10.1007/s12020-018-1678-1. Epub 2018 Jul 18. Endocrine. 2018. PMID: 30022382
-
Guidelines for the use of radio-iodine, thyroid hormone, and treatment of metastatic disease in patients with differentiated thyroid cancer.Surg Oncol Clin N Am. 1998 Oct;7(4):665-80. Surg Oncol Clin N Am. 1998. PMID: 9735128 Review.
-
[The basis for radioiodine therapy in differentiated thyroid cancer].Ther Umsch. 1999 Jul;56(7):403-7. doi: 10.1024/0040-5930.56.7.403. Ther Umsch. 1999. PMID: 10434780 Review. German.
Cited by
-
Mathematical models applied to thyroid cancer.Biophys Rev. 2019 Apr;11(2):183-189. doi: 10.1007/s12551-019-00504-7. Epub 2019 Feb 15. Biophys Rev. 2019. PMID: 30771157 Free PMC article. Review.
-
Radiation necrosis after radiation therapy treatment of brain metastases: A computational approach.PLoS Comput Biol. 2024 Jan 30;20(1):e1011400. doi: 10.1371/journal.pcbi.1011400. eCollection 2024 Jan. PLoS Comput Biol. 2024. PMID: 38289964 Free PMC article.
-
Appraisal of radioiodine refractory thyroid cancer: advances and challenges.Am J Cancer Res. 2020 Jul 1;10(7):1923-1936. eCollection 2020. Am J Cancer Res. 2020. PMID: 32774993 Free PMC article. Review.
-
Spatially fractionated GRID radiation potentiates immune-mediated tumor control.Radiat Oncol. 2024 Sep 13;19(1):121. doi: 10.1186/s13014-024-02514-6. Radiat Oncol. 2024. PMID: 39272128 Free PMC article.
-
Personalized treatment options for thyroid cancer: current perspectives.Pharmgenomics Pers Med. 2019 Sep 13;12:235-245. doi: 10.2147/PGPM.S181520. eCollection 2019. Pharmgenomics Pers Med. 2019. PMID: 31571972 Free PMC article. Review.
References
-
- Schlumberger M, Challeton C, De Vathaire F, Travagli JP, Gardet P, Lumbroso JD, Francese C, Fontaine F, Ricard M, Parmentier C. Radioactive iodine treatment and external radiotherapy for lung and bone metastases from thyroid carcinoma. J Nucl Med. 1996;37:598–605. - PubMed
-
- Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De Vathaire F, Schlumberger M. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91:2892–2899. - PubMed
-
- Lassmann M, Reiners C, Luster M. Dosimetry and thyroid cancer: the individual dosage of radioiodine. Endocr Relat Cancer. 2010;17:R161–172. - PubMed
-
- Deandreis D, Rubino C, Tala H, Leboulleux S, Terroir M, Baudin E, Larson S, Fagin JA, Schlumberger M, Tuttle MR. Comparison Of Empiric Versus Whole Body/Blood Clearance Dosimetry-Based Approach To Radioactive Iodine Treatment In Patients With Metastases From Differentiated Thyroid Cancer. J Nucl Med. 2016 - PubMed
-
- Hay ID, Gonzalez-Losada T, Reinalda MS, Honetschlager JA, Richards ML, Thompson GB. Long-term outcome in 215 children and adolescents with papillary thyroid cancer treated during 1940 through 2008. World J Surg. 2010;34:1192–1202. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
