

The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies
- PMID: 28390479
- PMCID: PMC5405702
- DOI: 10.1016/j.jaci.2017.01.011
The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies
Abstract
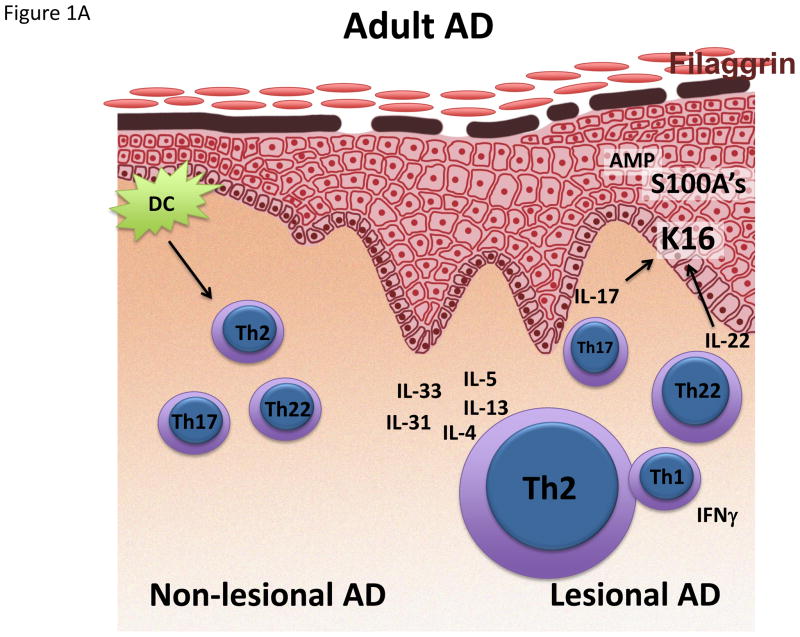
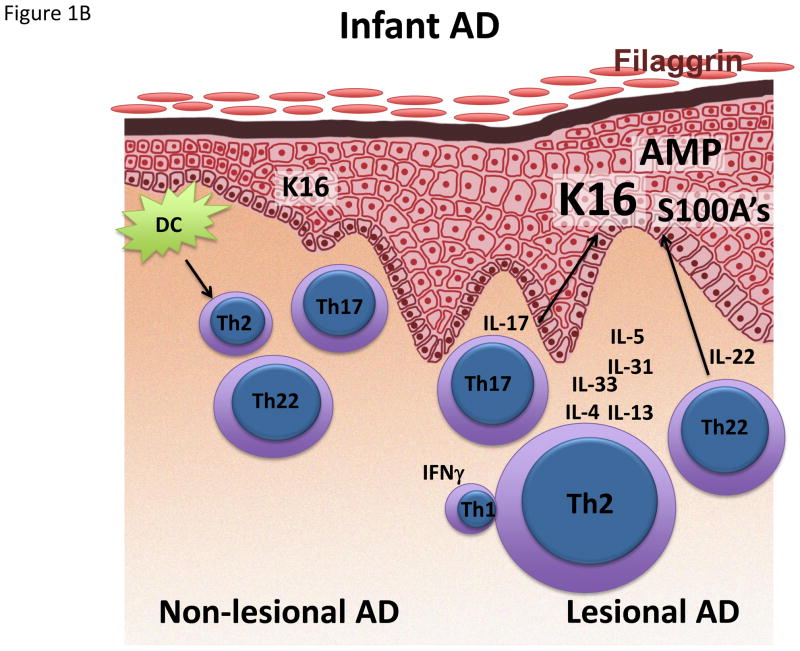
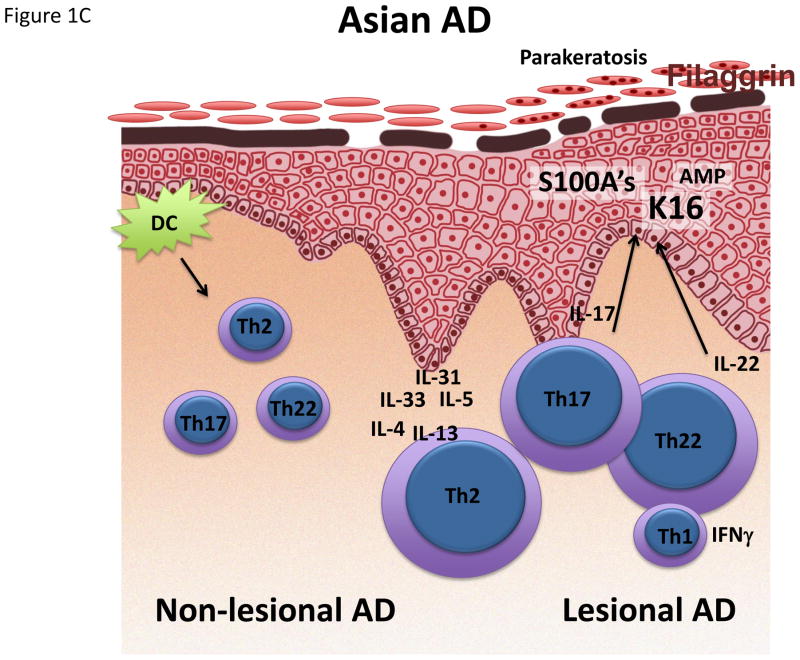
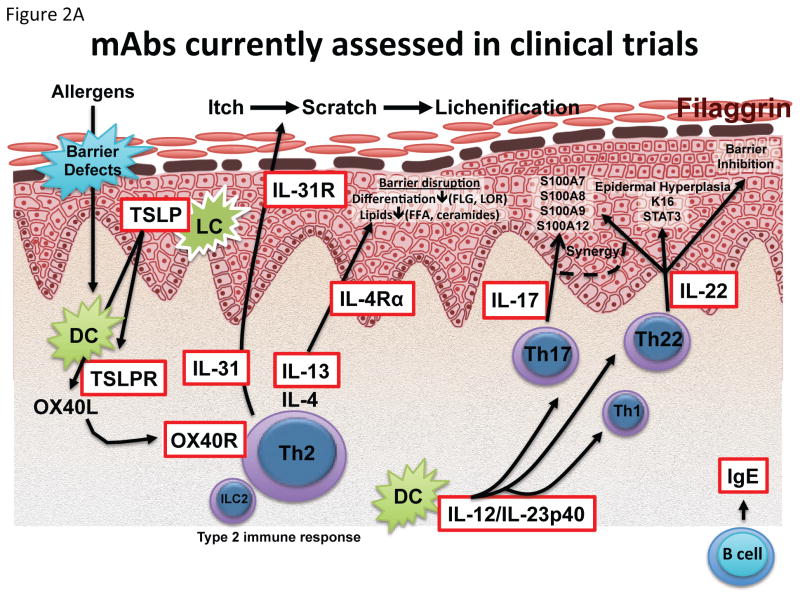
Atopic dermatitis (AD), the most common chronic inflammatory skin disease, is driven by both terminal keratinocyte differentiation defects and strong type 2 immune responses. In contrast to chronic plaque-type psoriasis, AD is now understood to be a much more heterogeneous disease, with additional activation of TH22, TH17/IL-23, and TH1 cytokine pathways depending on the subtype of the disease. In this review we discuss our current understanding of the AD immune map in both patients with early-onset and those with chronic disease. Clinical studies with broad and targeted therapeutics have helped to elucidate the contribution of various immune axes to the disease phenotype. Importantly, immune activation extends well beyond lesional AD because nonlesional skin and the blood component harbor AD-specific inflammatory changes. For this reason, future therapeutics will need to focus on a systemic treatment approach, especially in patients with moderate-to-severe disease.
Keywords: Atopic dermatitis; T helper cell; eczema; immune; keratinocyte; skin immune map; targeted therapy.
Copyright © 2017 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Hanifin JM, Reed ML, Eczema P Impact Working G. A population-based survey of eczema prevalence in the United States. Dermatitis. 2007;18:82–91. - PubMed
-
- Flohr C, Mann J. New insights into the epidemiology of childhood atopic dermatitis. Allergy. 2014;69:3–16. - PubMed
-
- Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387:1109–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
