

Pharmacist participation in hospital ward teams and hospital readmission rates among people with dementia: a randomized controlled trial
- PMID: 28391409
- PMCID: PMC5486919
- DOI: 10.1007/s00228-017-2249-8
Pharmacist participation in hospital ward teams and hospital readmission rates among people with dementia: a randomized controlled trial
Abstract
Purpose: To assess whether comprehensive medication reviews conducted by clinical pharmacists as part of a healthcare team reduce drug-related hospital readmission rates among people with dementia or cognitive impairment.
Methods: This randomized controlled trial was carried out between January 9, 2012, and December 2, 2014. Patients aged ≥65 years with dementia or cognitive impairment admitted to three wards at two hospitals located in Northern Sweden were included.
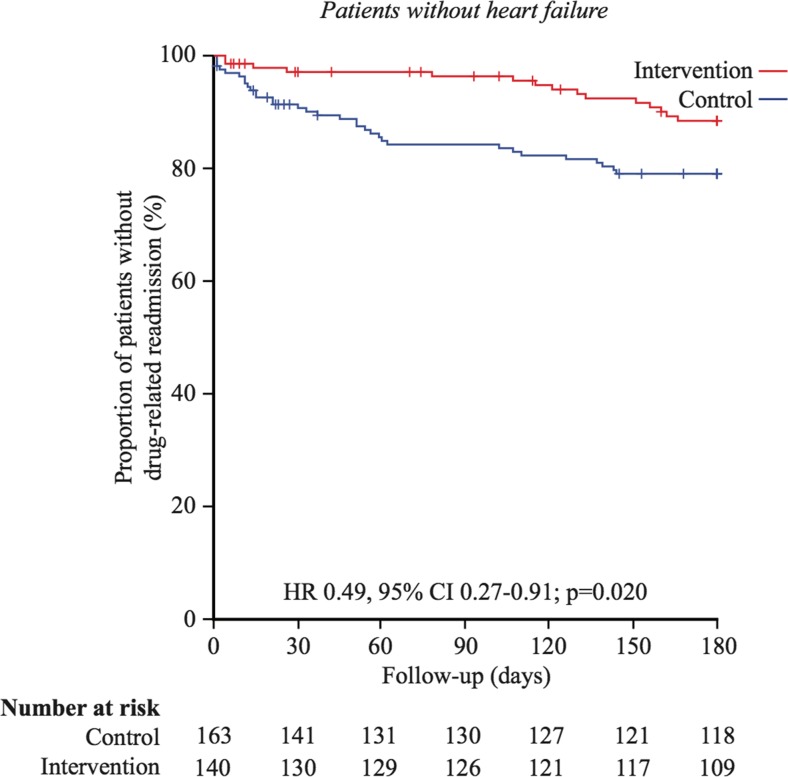
Results: Of the 473 deemed eligible for participation, 230 were randomized to intervention and 230 to control group by block randomization. The primary outcome, risk of drug-related hospital readmissions, was assessed at 180 days of follow-up by intention-to-treat analysis. During the 180 days of follow-up, 18.9% (40/212) of patients in the intervention group and 23.0% (50/217) of those in the control group were readmitted for drug-related reasons (HR = 0.80, 95% CI = 0.53-1.21, p = 0.28, univariable Cox regression). Heart failure was significantly more common in the intervention group. After adjustment for heart failure as a potential confounder and an interaction term, multiple Cox regression analysis indicated that pharmacist participation significantly reduced the risk of drug-related readmissions (HR = 0.49, 95% CI = 0.27-0.90, p = 0.02). A post-hoc analysis showed a significantly reduced risk of 30-day readmissions due to drug-related problems in the total sample (without adjustment for heart failure).
Conclusion: Participation of clinical pharmacists in healthcare team conducting comprehensive medication reviews did not significantly reduce the risk of drug-related readmissions in patients with dementia or cognitive impairment; however, post-hoc and subgroup analyses indicated significant effects favoring the intervention. More research is needed.
Trial registration: Clinical trials NCT01504672.
Keywords: Clinical pharmacists; Dementia; Drug-related readmissions; Medication reviews; Old people.
Conflict of interest statement
Description of authors’roles
All authors were involved in the study concept and design. Maria Gustafsson, Bettina Pfister, Jeanette Jonsson, and Hugo Lövheim were involved in the acquisition, analysis, and interpretation of data. Maria Gustafsson and Hugo Lövheim did the statistical analysis. All authors participated in the critical revision of the manuscript, contributed comments, and approved the final version.
Conflict of interest
The authors declare that they have no conflict of interest.
Figures




References
-
- Gillespie U, Alassaad A, Henrohn D, Garmo H, Hammarlund-Udenaes M, Toss H, Kettis-Lindblad A, Melhus H, Morlin C. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169:894–900. doi: 10.1001/archinternmed.2009.71. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
