

Femoral neck fracture osteosynthesis by the biplane double-supported screw fixation method (BDSF) reduces the risk of fixation failure: clinical outcomes in 207 patients
- PMID: 28391429
- PMCID: PMC5432592
- DOI: 10.1007/s00402-017-2689-8
Femoral neck fracture osteosynthesis by the biplane double-supported screw fixation method (BDSF) reduces the risk of fixation failure: clinical outcomes in 207 patients
Abstract
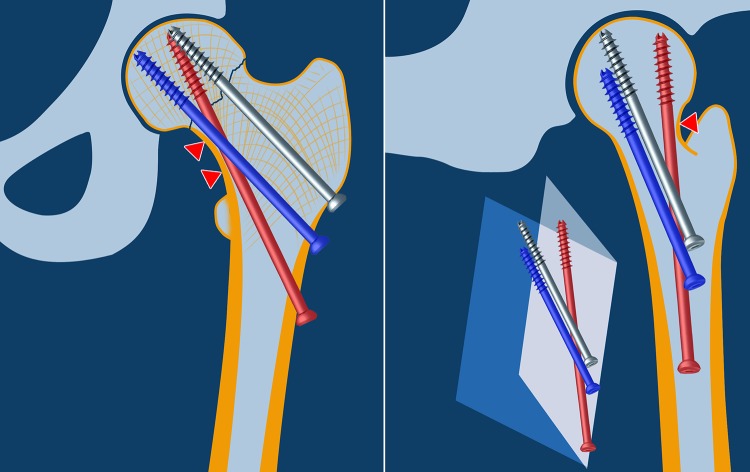
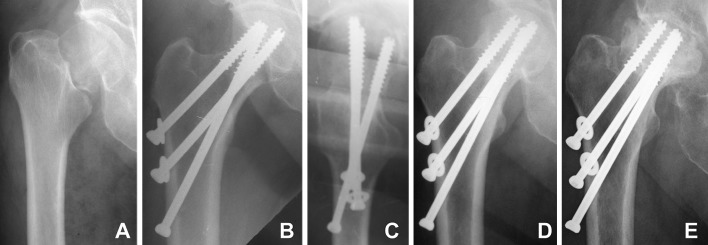
Introduction: Osteosynthesis of femoral neck fractures is related up to 46% rate of complications. The novel method of biplane double-supported screw fixation (BDSF; Filipov's method) offers better stability using three medially diverging cannulated screws with two of them buttressed on the calcar. Biomechanically, the most effective component is the distal screw placed at steeper angle and supported on a large area along the distal and posterior cortex of the femoral neck following its spiral anterior curve. Thereby, BDSF achieves the strongest possible distal-posterior cortical support for the fixation construct, which allows for immediate full weight-bearing. The aim of this study was to evaluate the outcomes from the first 5-year period of BDSF clinical application.
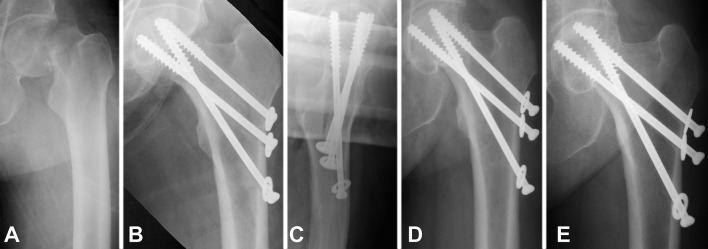
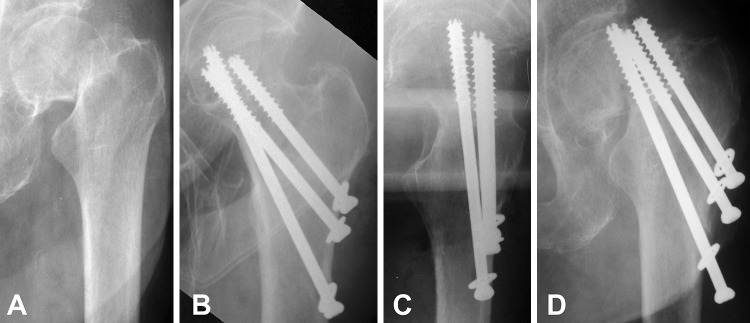
Materials and methods: Subject of this retrospective study were 207 patients with displaced Garden III-IV femoral neck fractures treated with BDSF. Three 7.3-mm cannulated screws were laid in two medially diverging oblique planes. The distal and the middle screws were supported on the calcar. The distal screw had additional support on the posterior neck cortex.
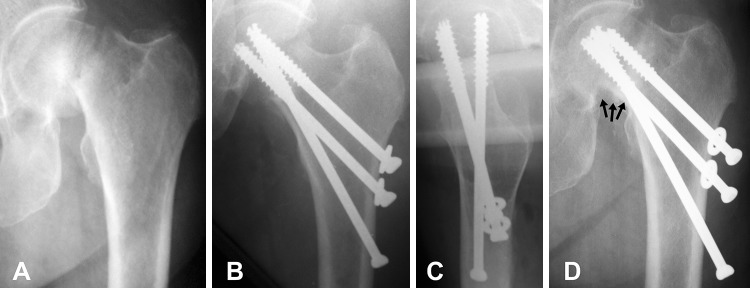
Results: The outcomes in 207 patients were analysed in 29.6 ± 16.8 months follow-up. Bone union occurred in 96.6% of the cases (males 97.6%, females 96.4%, P = 0.99). Rate of nonunion was 3.4%, including fixation failure (2.4%), pseudoarthrosis (0.5%) and nonunion with AVN (0.5%). Rate of AVN was 12.1% (males 4.8%, females 13.9%, P = 0.12). Modified Harris hip score was 86.2 ± 18.9 (range 10-100), with no significant difference between genders, P = 0.07. Older patients were admitted with significantly more comorbidities (P = 0.001), and on follow-up they were significantly less mobile (P = 0.005) and had significantly more difficulties to put socks and shoes on (P < 0.001).
Conclusions: By providing additional cortical support, the novel BDSF method enhances femoral neck fracture fixation strength.
Keywords: BDSF; Biplane; Femoral neck fracture; Fixation; Hip fractures; Osteosynthesis.
Conflict of interest statement
Conflict of interest
The author(s) declare that they have no competing interests.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study for their treatment choice.
Figures
Comment in
-
Letter to the Editor concerning "Femoral neck fracture osteosynthesis by the biplane double-supported screw fixation method (BDSF) reduces the risk of fixation failure: clinical outcomes in 207 patients" by Filipov O, Sommer C et al (2017). Arch Orthop Trauma Surg. Apr 8. (Epub ahead of print).Arch Orthop Trauma Surg. 2017 Aug;137(8):1165. doi: 10.1007/s00402-017-2710-2. Epub 2017 May 9. Arch Orthop Trauma Surg. 2017. PMID: 28488016 No abstract available.
-
Biomechanics and indications for application of the method of BDSF. Answer to manuscript draft number AOTS-D- 17-00378, Letter to the Editor concerning ''Femoral neck fracture osteosynthesis by the biplane double-supported screw fixation method (BDSF) reduces the risk of fixation failure: clinical outcomes in 207 patients'' by Filipov O, Sommer C, et al. (2017) Arch Orthop Trauma Surg. Apr 8. [Epub ahead of print].Arch Orthop Trauma Surg. 2017 Aug;137(8):1167-1171. doi: 10.1007/s00402-017-2716-9. Epub 2017 Jun 30. Arch Orthop Trauma Surg. 2017. PMID: 28667396 Free PMC article. No abstract available.
-
Response concerning 'Letter to editor' by Ni et al. (2017), Arch Orthop Trauma Surg. DOI 10.1007/s00402-017-2710-2.Arch Orthop Trauma Surg. 2017 Oct;137(10):1341. doi: 10.1007/s00402-017-2768-x. Epub 2017 Jul 29. Arch Orthop Trauma Surg. 2017. PMID: 28756585 No abstract available.
References
-
- Damany DS, Parker MJ, Chojnowski A. Complications after intracapsular hip fractures in young adults. A meta-analysis of 18 published studies involving 564 fractures. Injury. 2005;36(1):131–141. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
