

Radiofrequency vs Microwave Ablation After Neoadjuvant Transarterial Bland and Drug-Eluting Microsphere Chembolization for the Treatment of Hepatocellular Carcinoma
- PMID: 28392205
- PMCID: PMC5563480
- DOI: 10.1067/j.cpradiol.2017.02.006
Radiofrequency vs Microwave Ablation After Neoadjuvant Transarterial Bland and Drug-Eluting Microsphere Chembolization for the Treatment of Hepatocellular Carcinoma
Abstract
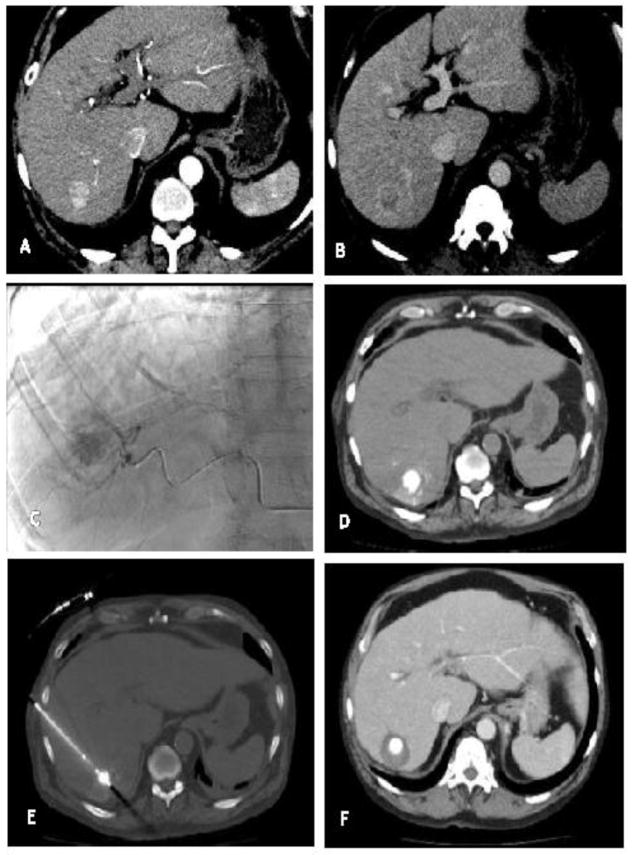
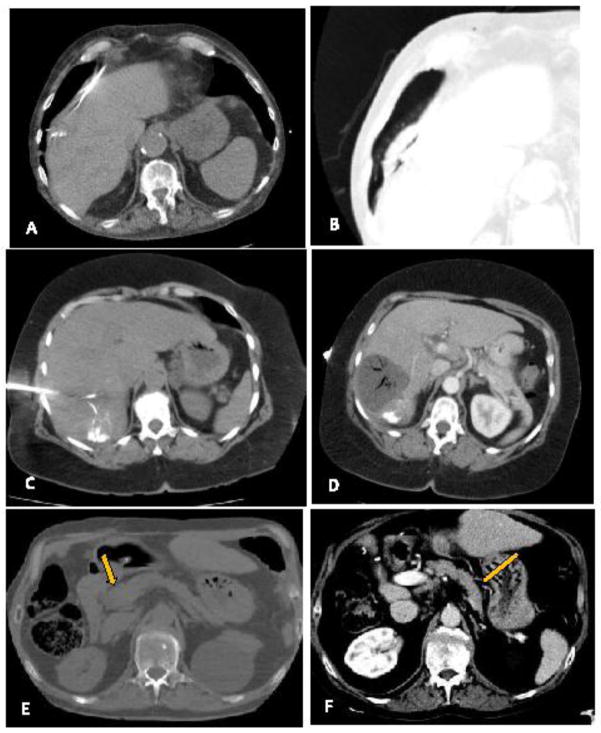
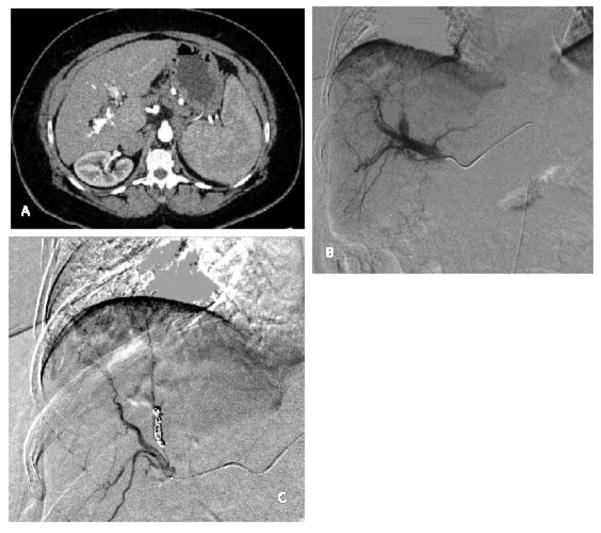
Aim: To retrospectively compare the initial response, local recurrence, and complication rates of radiofrequency ablation (RFA) vs microwave ablation (MWA) when combined with neoadjuvant bland transarterial embolization (TAE) or drug-eluting microsphere chemoembolization (TACE) for the treatment of hepatocellular carcinoma (HCC).
Methods: A total of 35 subjects with Barcelona Clinic Liver Cancer (BCLC) very early and early-stage HCC (range: 1.2-4.1cm) underwent TAE (23) or TACE (12) with RFA (15) or microwave ablation (MWA) (20) from January 2009 to June 2015 as either definitive therapy or a bridge to transplant. TAE and TACE were performed with 40-400μm particles and 30-100μm plus either doxorubicin- or epirubicin-eluting microspheres, respectively. Initial response and local progression were evaluated using modified response evaluation criteria in solid tumors. Complications were graded using common terminology criteria for adverse events version 5.0.
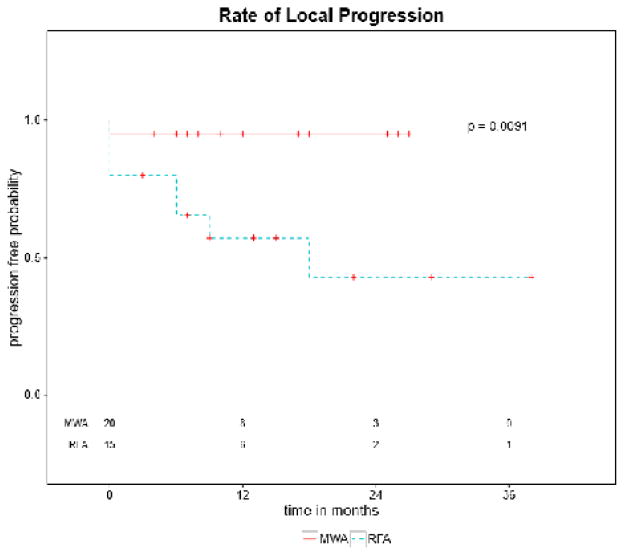
Results: Complete response rates were 80% (12/15) for RFA + TAE/TACE and 95% (19/20) for MWA + TAE/TACE (P = 0.29). Local recurrence rate was 30% (4/12) for RFA + TAE/TACE and 0% (0/19) for MWA + TAE/TACE. Durability of response, defined as local disease control for duration of the study, demonstrated a significant difference in favor of MWA (P = 0.0091). There was no statistical difference in complication rates (3 vs 2).
Conclusions: MWA and RFA when combined with neoadjuvant TAE or TACE have similar safety and efficacy in the treatment of early-stage HCC. MWA provided more durable disease control in this study; however, prospective data remain necessary to evaluate superiority of either modality.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: Beau Toskich became a consultant for Neuwave Medical subsequent to the collection and analysis of this data. All other authors have no conflicts of interest to disclose.
Figures


References
-
- Kirk A. Textbook of organ transplantation. Chichester, West Sussex: John Wiley & Sons, Inc; 2014.
-
- Cabrera R, Dhanasekaran R, Caridi J, Clark V, Morelli G, Soldevila-Pico C, et al. Impact of transarterial therapy in hepatitis C-related hepatocellular carcinoma on long-term outcomes after liver transplantation. Am J Clin Oncol. 2012;35(4):345–50. doi: 10.1097/COC.0b013e31821631f6. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
