

Should nurses be allowed to perform the pre-operative surgical site marking instead of surgeons? A prospective feasibility study at a Swiss primary care teaching hospital
- PMID: 28392834
- PMCID: PMC5379652
- DOI: 10.1186/s13037-017-0125-1
Should nurses be allowed to perform the pre-operative surgical site marking instead of surgeons? A prospective feasibility study at a Swiss primary care teaching hospital
Abstract
Background: Surgical site marking is one important cornerstone for the principles of safe surgery suggested by the WHO. Generally it is recommended that the attending surgeon performs the surgical site marking. Particularly in the case of same day surgery, this recommendation is almost not feasible. Therefore we systematically monitored, whether surgical site marking can be performed by trained nursing staff. The aim of the study was to find out whether surgical site marking can be carried out reliably and correctly by nurses.
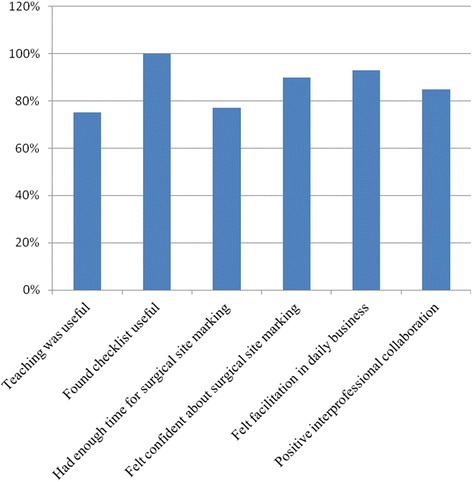
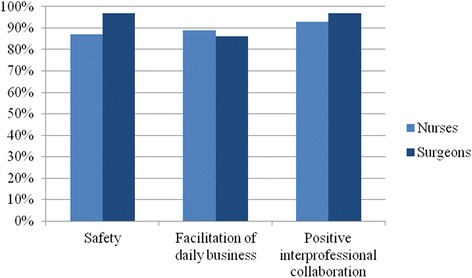
Methods: The prospective non-controlled interventional study took place in a single primary care hospital of Uster in Switzerland. During a pilot phase of 3 months (starting October 2012) the nursing staff of a single ward was trained and applied the surgical site marking on behalf of the responsible surgeon. After this initial phase the new concept was introduced in the entire surgical department. 12 months after the introduction of the new concept an interim evaluation was performed asking whether the new process facilitates daily routine and surgical site marking was performed correctly. 22 months after the introduction a prospective data collection monitored for one month whether the nursing staff carried out surgical site marking independently and correctly. Data were collected by a patient-accompanying checklist that was completed by the nursing staff, the staff in the operating room and the responsible surgeons.
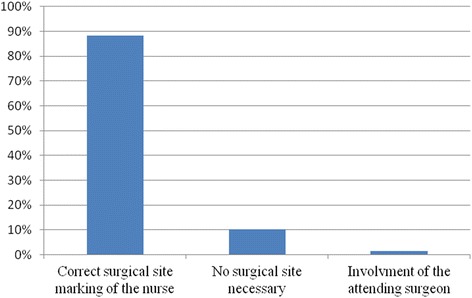
Results: The stepwise implementation of the new concept of surgical site marking was well accepted by the entire staff. 150 patient-accompanying checklists were analyzed. 22 data sheets were excluded from the analysis. 90% (n = 115/128) of the surgical site markings were correctly performed. For the remaining 10% either a surgical site marking was not necessary or the nursing staff asked a surgeon to mark the correct surgical site. During the whole study time of almost 3 years, no wrong-site surgery occurred.
Conclusion: Surgical site marking can be performed by trained nurses. However, the attending surgeon remains fully responsible of the correct operation on the correct patient.
Keywords: Implementation; Safety; Surgery; Surgical site marking; Time-out; Wrong-site surgery.
Figures

Similar articles
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and pre-registration house officers in pre-operative assessment in elective general surgery.Health Technol Assess. 2001;5(20):1-87. doi: 10.3310/hta5200. Health Technol Assess. 2001. PMID: 11427189 Clinical Trial.
-
Tune-In and Time-Out: Toward Surgeon-Led Prevention of "Never" Events.J Patient Saf. 2019 Dec;15(4):e36-e39. doi: 10.1097/PTS.0000000000000259. J Patient Saf. 2019. PMID: 26756728
-
Using "near misses" analysis to prevent wrong-site surgery.J Healthc Qual. 2015 Mar-Apr;37(2):126-32. doi: 10.1111/jhq.12037. J Healthc Qual. 2015. PMID: 24033453
-
Wrong-Site Surgery in Pediatric Ophthalmology.J Pediatr Ophthalmol Strabismus. 2018 May 1;55(3):152-158. doi: 10.3928/01913913-20180220-02. J Pediatr Ophthalmol Strabismus. 2018. PMID: 29796679 Review.
-
"Team time-out" and surgical safety-experiences in 12,390 neurosurgical patients.Neurosurg Focus. 2012 Nov;33(5):E6. doi: 10.3171/2012.8.FOCUS12261. Neurosurg Focus. 2012. PMID: 23116101 Review.
Cited by
-
Surgeons, sign your site!Patient Saf Surg. 2017 Apr 4;11:8. doi: 10.1186/s13037-017-0122-4. eCollection 2017. Patient Saf Surg. 2017. PMID: 28392833 Free PMC article.
-
Intraoperative practices to prevent wrong-level spine surgery: a survey among 105 spine surgeons in the United Kingdom.Patient Saf Surg. 2022 Jan 26;16(1):6. doi: 10.1186/s13037-021-00310-9. Patient Saf Surg. 2022. PMID: 35081968 Free PMC article.
References
-
- Stahel PF, Sabel AL, Victoroff MS, Varnell J, Lembitz A, Boyle DJ, Clarke TJ, Smith WR, Mehler PS. Wrong-site and wrong-patient procedures in the universal protocol era: analysis of a prospective database of physician self-reported occurrences. Arch Surg. 2010;145:978–84. doi: 10.1001/archsurg.2010.185. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
