

Coagulopathies in cyanotic cardiac patients: An analysis with three point - of - care testing devices (Thromboelastography, rotational thromboelastometry, and sonoclot analyzer)
- PMID: 28393783
- PMCID: PMC5408528
- DOI: 10.4103/aca.ACA_4_17
Coagulopathies in cyanotic cardiac patients: An analysis with three point - of - care testing devices (Thromboelastography, rotational thromboelastometry, and sonoclot analyzer)
Abstract
Introduction: In the last few years, viscoelastic point-of-care (POC) coagulation devices such as thromboelastography (TEG), rotational thromboelastometry (ROTEM), and Sonoclot (SON) analyzer have been increasingly used in major surgeries for timely assessment and management of coagulopathies. The aim of the present study was to evaluate coagulation profile of cyanotic cardiac patients with TEG, ROTEM, and SON analyzer. In addition, we assessed the correlation of standard laboratory coagulation tests and postoperative chest drain output (CDO) with the parameters of POC testing devices.
Materials and methods: Thirty-five patients of either gender, belonging to the American Society of Anesthesiologists Grade I-III, and undergoing elective cardiac surgery on cardiopulmonary bypass for cyanotic congenital heart disease were included in this study. To identify possible coagulation abnormalities, blood samples for TEG, ROTEM, SON, and standard laboratory coagulation were collected after induction of anesthesia. The correlations between variables were assessed using Pearson's correlation coefficient. P < 0.05 was considered statistically significant.
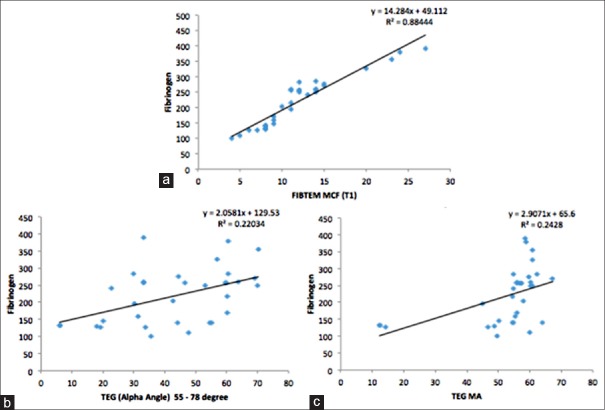
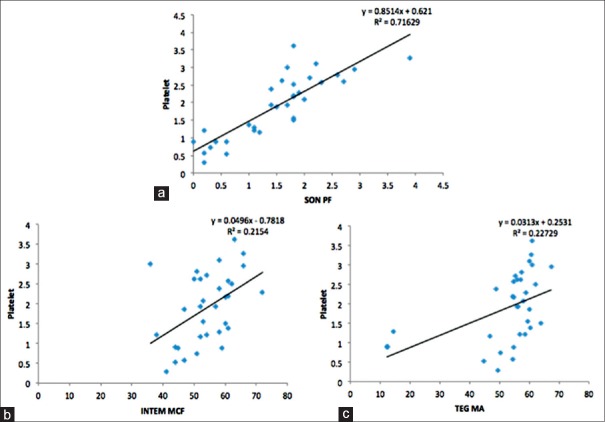
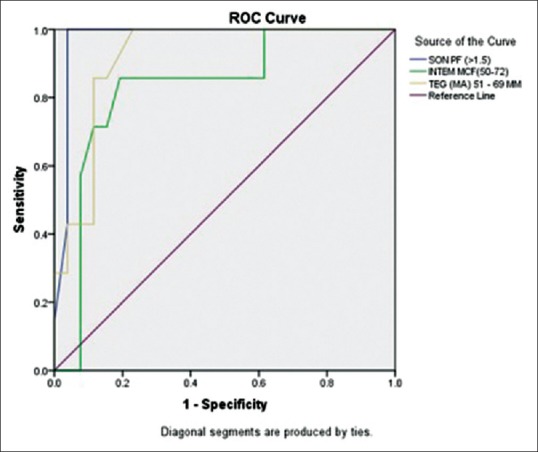
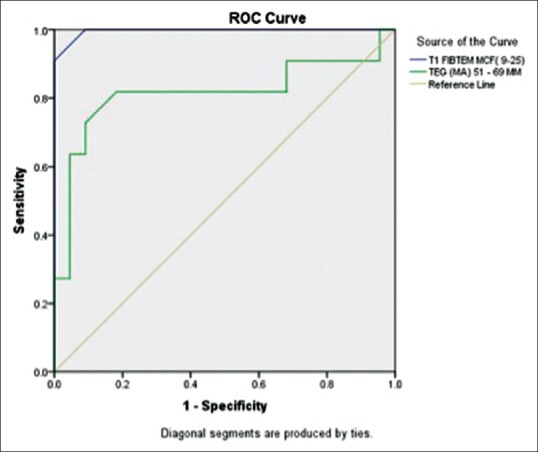
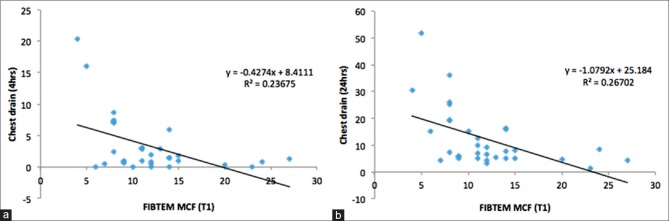
Results and discussion: EXTEM clot time (CT) and clot formation time (CFT) were prolonged in 87% and 45% patients whereas INTEM CT and CFT were prolonged in 36% and 73% patients, respectively. FIBTEM maximum clot firmness (MCF) was decreased in 30% patients. We observed significant correlation between fibrinogen concentration and ROTEM FIBTEM MCF (r = 0.94, P < 0.001). The SON platelet function (SON PF) showed good correlation with platelet count (r = 0.85, P < 0.001). We also found significant correlation between preoperative FIBTEM MCF and CDO in first 4 postoperative hours (r = 0.49, P = 0.004) and 24 postoperative hours (r = 0.52, P = 0.005). Receiver operating characteristic analysis demonstrated that SON PF and TEG maximum amplitude are highly predictive of thrombocytopenia below 100 × 109/L (area under the curve [AUC] - 0.97 and 0.92, respectively), while FIBTEM-MCF is highly predictive of hypofibrinogenemia (fibrinogen <150 mg/dL (AUC, 0.99).
Conclusion: Cyanotic cardiac patients have preoperative coagulation abnormalities in ROTEM, TEG, and SON parameters. ROTEM FIBTEM is highly predictive of hypofibrinogenemia while SON PF is highly predictive of thrombocytopenia. ROTEM FIBTEM can be studied as a marker of increased postoperative CDO.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Ghasemi A, Horri M, Salahshour Y. Coagulation abnormalities in pediatric patients with congenital heart disease: A literature review. Int J Pediatr. 2014;2:141–3.
-
- Horigome H, Hiramatsu Y, Shigeta O, Nagasawa T, Matsui A. Overproduction of platelet microparticles in cyanotic congenital heart disease with polycythemia. J Am Coll Cardiol. 2002;39:1072–7. - PubMed
-
- Despotis GJ, Gravlee G, Filos K, Levy J. Anticoagulation monitoring during cardiac surgery: A review of current and emerging techniques. Anesthesiology. 1999;91:1122–51. - PubMed
-
- Bolliger D, Szlam F, Levy JH, Molinaro RJ, Tanaka KA. Haemodilution-induced profibrinolytic state is mitigated by fresh-frozen plasma: Implications for early haemostatic intervention in massive haemorrhage. Br J Anaesth. 2010;104:318–25. - PubMed
-
- Nuttall GA, Oliver WC, Ereth MH, Santrach PJ. Coagulation tests predict bleeding after cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 1997;11:815–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical