

Tau-PET Binding Distinguishes Patients With Early-stage Posterior Cortical Atrophy From Amnestic Alzheimer Disease Dementia
- PMID: 28394771
- PMCID: PMC5443698
- DOI: 10.1097/WAD.0000000000000196
Tau-PET Binding Distinguishes Patients With Early-stage Posterior Cortical Atrophy From Amnestic Alzheimer Disease Dementia
Abstract
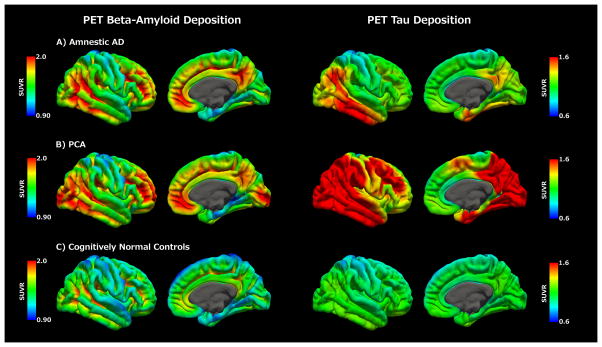
Background: Flortaucipir (tau) positron emission tomography (PET) binding distinguishes individuals with clinically well-established posterior cortical atrophy (PCA) due to Alzheimer disease (AD) from cognitively normal (CN) controls. However, it is not known whether tau-PET binding patterns differentiate individuals with PCA from those with amnestic AD, particularly early in the symptomatic stages of disease.
Methods: Flortaucipir and florbetapir (β-amyloid) PET imaging were performed in individuals with early-stage PCA (N=5), amnestic AD dementia (N=22), and CN controls (N=47). Average tau and β-amyloid deposition were quantified using standard uptake value ratios and compared at a voxelwise level, controlling for age.
Results: PCA patients [median age-at-onset, 59 (51 to 61) years] were younger at symptom onset than similarly staged individuals with amnestic AD [75 (60 to 85) years] or CN controls [73 (61 to 90) years; P=0.002]. Flortaucipir uptake was higher in individuals with early-stage symptomatic PCA versus those with early-stage amnestic AD or CN controls, and greatest in posterior regions. Regional elevations in florbetapir were observed in areas of greatest tau deposition in PCA patients.
Conclusions and relevance: Flortaucipir uptake distinguished individuals with PCA and amnestic AD dementia early in the symptomatic course. The posterior brain regions appear to be uniquely vulnerable to tau deposition in PCA, aligning with clinical deficits that define this disease subtype.
Figures


Similar articles
-
Relationships between flortaucipir PET tau binding and amyloid burden, clinical diagnosis, age and cognition.Brain. 2017 Mar 1;140(3):748-763. doi: 10.1093/brain/aww334. Brain. 2017. PMID: 28077397 Free PMC article.
-
Comparison of imaging biomarkers for Alzheimer's disease: amyloid imaging with [18F]florbetapir positron emission tomography and magnetic resonance imaging voxel-based analysis for entorhinal cortex atrophy.Int J Geriatr Psychiatry. 2015 May;30(5):505-13. doi: 10.1002/gps.4173. Epub 2014 Jul 7. Int J Geriatr Psychiatry. 2015. PMID: 25043833
-
Association of APOE4 and Clinical Variability in Alzheimer Disease With the Pattern of Tau- and Amyloid-PET.Neurology. 2021 Feb 2;96(5):e650-e661. doi: 10.1212/WNL.0000000000011270. Epub 2020 Dec 1. Neurology. 2021. PMID: 33262228 Free PMC article.
-
Perspectives and a Systematic Scoping Review on Longitudinal Profiles of Posterior Cortical Atrophy Syndrome.Curr Neurol Neurosci Rep. 2022 Nov;22(11):803-812. doi: 10.1007/s11910-022-01238-y. Epub 2022 Oct 15. Curr Neurol Neurosci Rep. 2022. PMID: 36242715
-
Early-onset Alzheimer Disease and Its Variants.Continuum (Minneap Minn). 2019 Feb;25(1):34-51. doi: 10.1212/CON.0000000000000687. Continuum (Minneap Minn). 2019. PMID: 30707186 Free PMC article. Review.
Cited by
-
Soluble amyloid-beta buffering by plaques in Alzheimer disease dementia versus high-pathology controls.PLoS One. 2018 Jul 6;13(7):e0200251. doi: 10.1371/journal.pone.0200251. eCollection 2018. PLoS One. 2018. PMID: 29979775 Free PMC article.
-
Visual Dysfunction in Posterior Cortical Atrophy.Front Neurol. 2017 Aug 16;8:389. doi: 10.3389/fneur.2017.00389. eCollection 2017. Front Neurol. 2017. PMID: 28861031 Free PMC article. Review.
-
Benson's Disease or Posterior Cortical Atrophy, Revisited.J Alzheimers Dis. 2021;82(2):493-502. doi: 10.3233/JAD-210368. J Alzheimers Dis. 2021. PMID: 34057092 Free PMC article. Review.
-
Widespread distribution of tauopathy in preclinical Alzheimer's disease.Neurobiol Aging. 2018 Dec;72:177-185. doi: 10.1016/j.neurobiolaging.2018.08.022. Epub 2018 Sep 1. Neurobiol Aging. 2018. PMID: 30292840 Free PMC article.
-
Posterior cortical atrophy: A rare variant of Alzheimer's disease.Neurol Int. 2018 May 24;10(2):7665. doi: 10.4081/ni.2018.7665. eCollection 2018 May 24. Neurol Int. 2018. PMID: 30069290 Free PMC article.
References
-
- Renner JA, Burns JM, Hou CE, McKeel DW, Jr, Storandt M, Morris JC. Progressive posterior cortical dysfunction: a clinicopathologic series. Neurology. 2004;63(7):1175–1180. - PubMed
-
- Tang-Wai DF, Graff-Radford NR, Boeve BF, et al. Clinical, genetic, and neuropathologic characteristics of posterior cortical atrophy. Neurology. 2004;63(7):1168–1174. - PubMed
-
- Crutch SJ, Schott JM, Rabinovici GD, et al. Shining a light on posterior cortical atrophy. Alzheimers Dement. 2013;9(4):463–465. - PubMed
-
- Benson DF, Davis RJ, Snyder BD. Posterior cortical atrophy. Arch Neurol. 1988;45(7):789–793. - PubMed
-
- Alladi S, Xuereb J, Bak T, et al. Focal cortical presentations of Alzheimer’s disease. Brain. 2007;130(Pt 10):2636–2645. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
