

Oxygen and oxidative stress in the perinatal period
- PMID: 28395175
- PMCID: PMC5388914
- DOI: 10.1016/j.redox.2017.03.011
Oxygen and oxidative stress in the perinatal period
Abstract
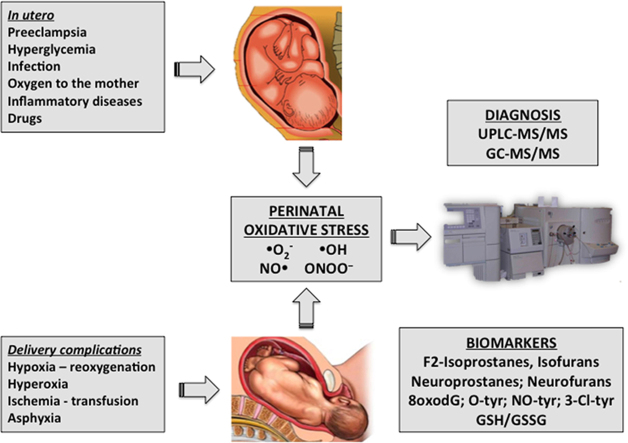
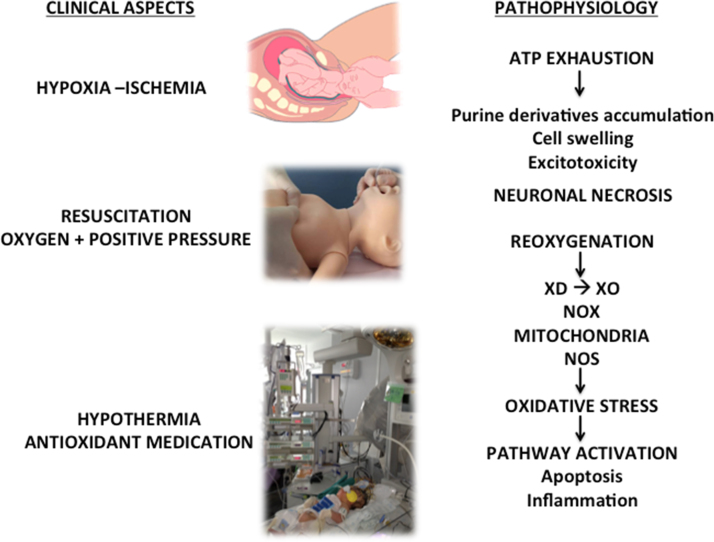
Fetal life evolves in a hypoxic environment. Changes in the oxygen content in utero caused by conditions such as pre-eclampsia or type I diabetes or by oxygen supplementation to the mother lead to increased free radical production and correlate with perinatal outcomes. In the fetal-to-neonatal transition asphyxia is characterized by intermittent periods of hypoxia ischemia that may evolve to hypoxic ischemic encephalopathy associated with neurocognitive, motor, and neurosensorial impairment. Free radicals generated upon reoxygenation may notably increase brain damage. Hence, clinical trials have shown that the use of 100% oxygen given with positive pressure in the airways of the newborn infant during resuscitation causes more oxidative stress than using air, and increases mortality. Preterm infants are endowed with an immature lung and antioxidant system. Clinical stabilization of preterm infants after birth frequently requires positive pressure ventilation with a gas admixture that contains oxygen to achieve a normal heart rate and arterial oxygen saturation. In randomized controlled trials the use high oxygen concentrations (90% to 100%) has caused more oxidative stress and clinical complications that the use of lower oxygen concentrations (30-60%). A correlation between the amount of oxygen received during resuscitation and the level of biomarkers of oxidative stress and clinical outcomes was established. Thus, based on clinical outcomes and analytical results of oxidative stress biomarkers relevant changes were introduced in the resuscitation policies. However, it should be underscored that analysis of oxidative stress biomarkers in biofluids has only been used in experimental and clinical research but not in clinical routine. The complexity of the technical procedures, lack of automation, and cost of these determinations have hindered the routine use of biomarkers in the clinical setting. Overcoming these technical and economical difficulties constitutes a challenge for the immediate future since accurate evaluation of oxidative stress would contribute to improve the quality of care of our neonatal patients.
Keywords: Biomarkers; High-risk pregnancy; Ischemia-reperfusion; Newborn; Oxidative stress; Oxygen.
Copyright © 2017 The Authors. Published by Elsevier B.V. All rights reserved.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
