Reirradiation of head and neck cancer in the era of intensity-modulated radiotherapy: patient selection, practical aspects, and current evidence
- PMID: 28395502
- PMCID: PMC5398346
- DOI: 10.3857/roj.2017.00122
Reirradiation of head and neck cancer in the era of intensity-modulated radiotherapy: patient selection, practical aspects, and current evidence
Abstract
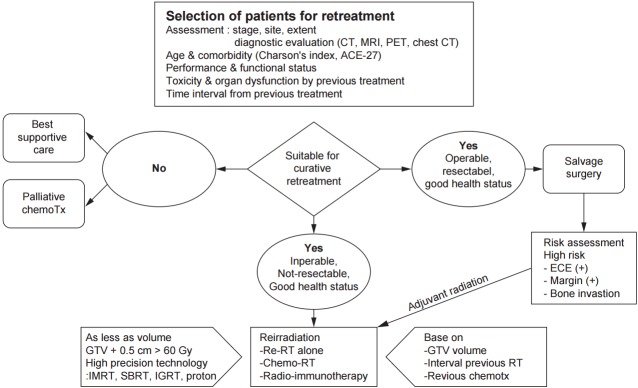
Locoregional failure is the most frequent pattern of failure in locally advanced head and neck cancer patients and it leads to death in most of the patients. Second primary tumors occurring in the other head and neck region reach up to almost 40% of long-term survivors. Recommended and preferred retreatment option in operable patients is salvage surgical resection, reporting a 5-year overall survival of up to 40%. However, because of tumor location, extent, and underlying comorbidities, salvage surgery is often limited and compromised by incomplete resection. Reirradiation with or without combined chemotherapy is an appropriate option for unresectable recurrence. Reirradiation is carefully considered with a case-by-case basis. Reirradiation protocol enrollment is highly encouraged prior to committing patient to an aggressive therapy. Radiation doses greater than 60 Gy are usually recommended for successful salvage. Despite recent technical improvement in intensity-modulated radiotherapy (IMRT), the use of concurrent chemotherapy, and the emergence of molecularly targeted agents, careful patient selection remain as the most paramount factor in reirradiation. Tumors that recur or persist despite aggressive prior chemoradiation therapy imply the presence of chemoradio-resistant clonogens. Treatment protocols that combine novel targeted radiosensitizing agents with conformal high precision radiation are required to overcome the resistance while minimizing toxicity. Recent large number of data showed that IMRT may provide better locoregional control with acceptable acute or chronic morbidities. However, additional prospective studies are required before a definitive conclusion can be drawn on safety and effectiveness of IMRT.
Keywords: Head and Neck neoplasms; Intensity-modulation radiation therapy (IMRT); Reirradiation; Toxicities.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Brockstein B, Haraf DJ, Rademaker AW, et al. Patterns of failure, prognostic factors and survival in locoregionally advanced head and neck cancer treated with concomitant chemoradiotherapy: a 9-year, 337-patient, multi-institutional experience. Ann Oncol. 2004;15:1179–86. - PubMed
-
- Cooper JS, Pajak TF, Rubin P, et al. Second malignancies in patients who have head and neck cancer: incidence, effect on survival and implications based on the RTOG experience. Int J Radiat Oncol Biol Phys. 1989;17:449–56. - PubMed
-
- Bachar GY, Goh C, Goldstein DP, O'Sullivan B, Irish JC. Long-term outcome analysis after surgical salvage for recurrent tonsil carcinoma following radical radiotherapy. Eur Arch Otorhinolaryngol. 2010;267:295–301. - PubMed
-
- Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359:1116–27. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical