

Avoidable costs of stenting for aortic coarctation in the United Kingdom: an economic model
- PMID: 28395657
- PMCID: PMC5387244
- DOI: 10.1186/s12913-017-2215-2
Avoidable costs of stenting for aortic coarctation in the United Kingdom: an economic model
Abstract
Background: Undesirable outcomes in health care are associated with patient harm and substantial excess costs. Coarctation of the aorta (CoA), one of the most common congenital heart diseases, can be repaired with stenting but requires monitoring and subsequent interventions to detect and treat disease recurrence and aortic wall injuries. Avoidable costs associated with stenting in patients with CoA are unknown.
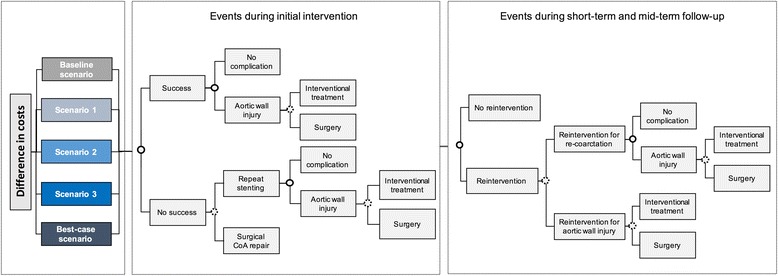
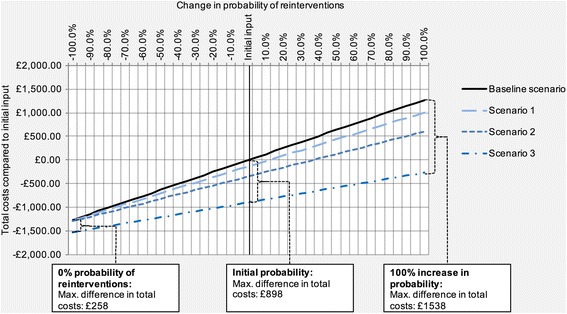
Methods: We developed an economic model to calculate potentially avoidable costs in stenting treatment of CoA in the United Kingdom over 5 years. We calculated baseline costs for the intervention and potentially avoidable complications and follow-up interventions and compared these to the costs in hypothetical scenarios with improved treatment effectiveness and complication rates.
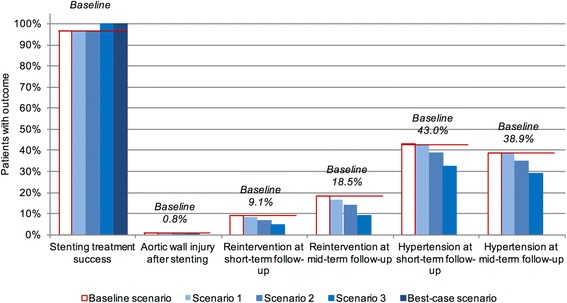
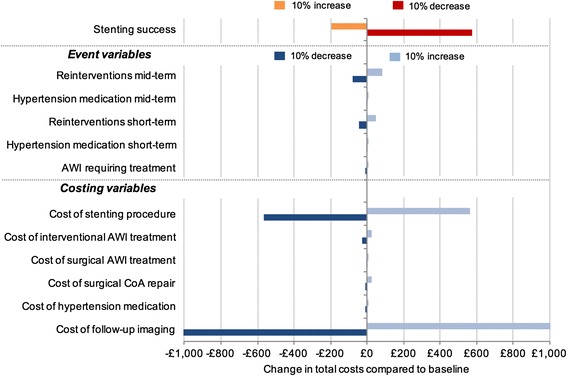
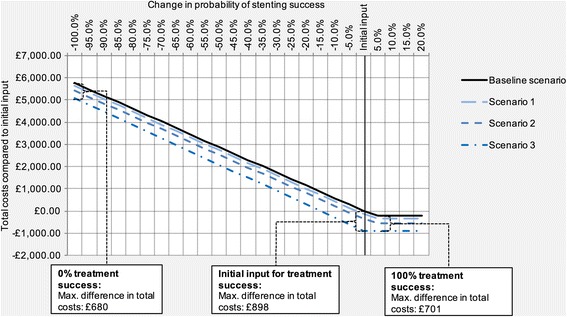
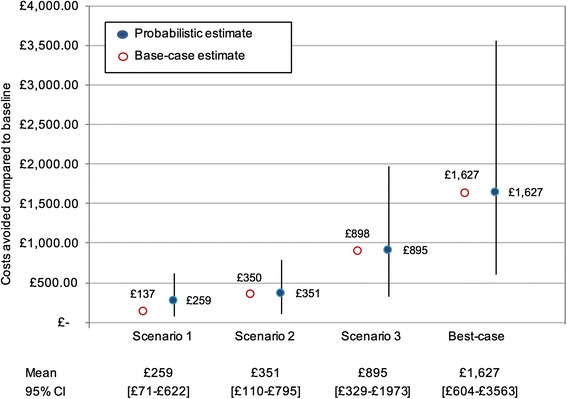
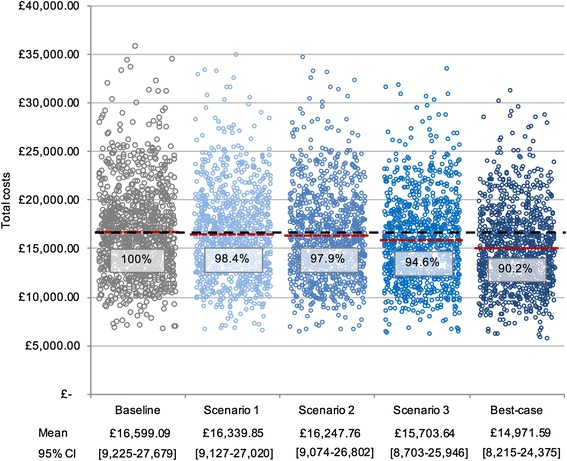
Results: Baseline costs were £16 688 ($25 182) per patient. Avoidable costs ranged from £137 ($207) per patient in a scenario assuming a 10% reduction in aortic wall injuries and reinterventions at follow-up, to £1627 ($2455) in a Best-case scenario with 100% treatment success and no complications. Overall costs in the Best-case scenario were 90.2% of overall costs at Baseline. Reintervention rate at follow-up was identified as most influential lever for overall costs. Probabilistic sensitivity analysis showed a considerable degree of uncertainty for avoidable costs with widely overlapping 95% confidence intervals.
Conclusions: Significant improvements in the treatment effectiveness and reductions in complication rates are required to realize discernible cost savings. Up to 10% of total baseline costs could be avoided in the best-case scenario. This highlights the need to pursue patient-specific treatment approaches which promise optimal outcomes.
Keywords: Avoidable costs; Coarctation of the aorta; Congenital; Cost savings; Heart defects; Stents.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
